Opening
Something brought you here. Maybe it was a documentary, a friend's account, a research paper, a decade of depression that conventional treatment hasn't touched. Whatever the reason, you've done enough to take this seriously — and that already puts you in a different category from someone who decides to take a large dose of psilocybin at a music festival and calls it therapy.
This module will not tell you that psychedelic therapy will change your life. That would be both premature and, in the wrong hands, dangerous. What it will do is give you an honest accounting of what we actually know — what the research shows, what it doesn't, what happens in real retreat settings versus what gets emphasized in media coverage, and what the five major medicines do differently. The goal is not to talk you into or out of anything. It's to ensure that whatever decision you make, you make it clearly.
There's a specific kind of magical thinking that circulates in psychedelic spaces — the idea that the medicine will do the work for you, that insight alone produces change, that a single session can undo decades of conditioning. This isn't entirely wrong. These experiences can be genuinely profound. But they are also demanding, sometimes destabilizing, occasionally frightening, and often more subtle in their long-term effects than the acute experience suggests. The people who do best are not the ones who arrived most convinced it would work. They're the ones who arrived most prepared.
Start here. Get a clear picture of what you're actually getting into. Everything else in this course builds on this foundation.
What Psychedelic Therapy Actually Is — and Isn't
The phrase "psychedelic therapy" covers a wide range of experiences that have almost nothing in common structurally except the use of a psychoactive compound. The most important thing to understand is the three-part structure that distinguishes therapy from simply taking a substance.
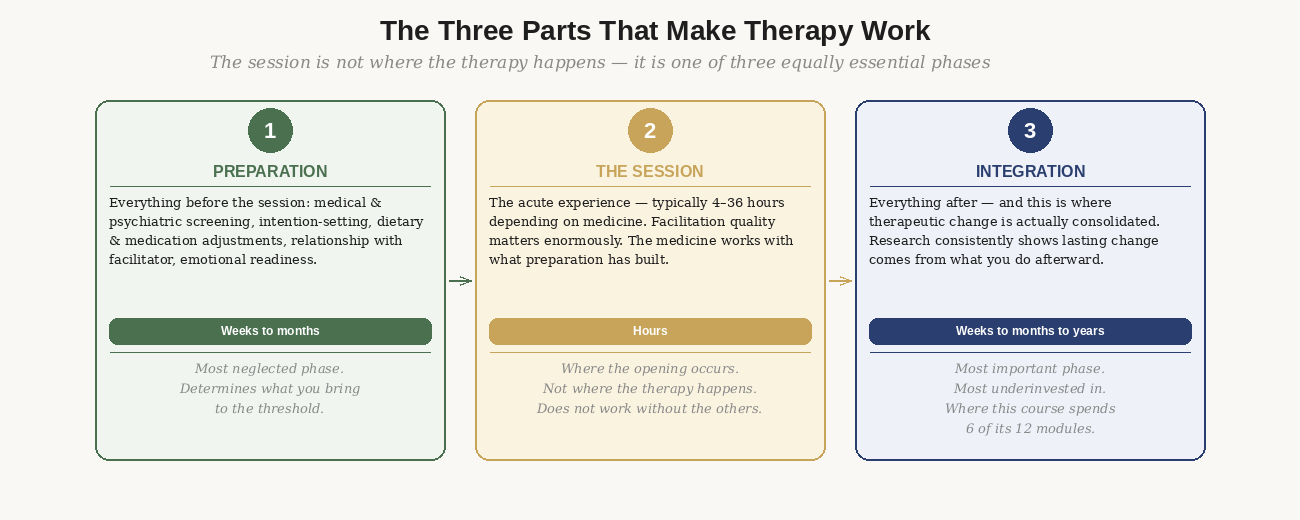
Figure 1: The three parts that make psychedelic therapy work. The session is not where the therapy happens — it is one of three equally essential phases. Most people invest heavily in the session and almost nothing in the other two.
What psychedelic therapy shares across its many forms is the fundamental mechanism: a psychoactive compound is used within a supported context with the intention of producing lasting psychological or behavioral change. The supported context — preparation, facilitation, and integration — is what distinguishes therapy from recreational use. Without that container, you may still have a powerful experience. But the evidence for therapeutic benefit is specific to structured, supported contexts.
Psychedelic therapy is not a cure, not guaranteed to be positive, not a shortcut, and not for everyone. The research is genuinely promising — and it is not proof that it will work for you specifically.
Integration — what you do in the weeks and months after the session — is where lasting change is actually produced. The session opens a window. Integration is what you build while it's open. This course spends six of its twelve modules on integration because that is where most people underinvest most dramatically.
The Spectrum: Recreational to Clinical
When evaluating your options, one of the most useful frameworks is understanding where different approaches sit on the spectrum from fully recreational to fully clinical. The word "retreat" itself guarantees nothing — quality varies enormously within that category.
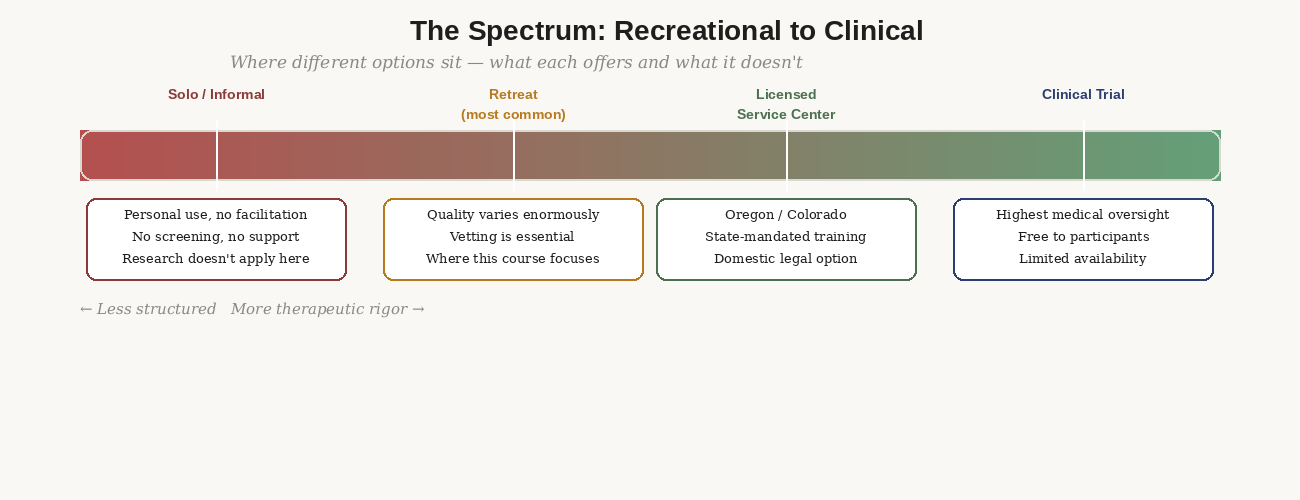
Figure 2: The spectrum from recreational to clinical. Each point on the spectrum has different levels of screening, facilitation quality, and integration support. Most people's options sit in the middle.
Most people reading this will pursue a retreat. The guidance in this course is designed for retreat programs that include at minimum: a medical intake process, preparation support, and integration circles afterward. If the program you're considering doesn't have all three, that's worth pausing on before booking.
A note on online ketamine
The rapid expansion of at-home ketamine services (Mindbloom, Joyous, etc.) deserves specific mention. These programs offer ketamine-assisted therapy without in-person supervision, which represents a very different risk profile from clinical ketamine treatment. They can be appropriate for certain presentations — particularly treatment-resistant depression — but the lack of in-person monitoring and the variation in integration support across providers means the standards in Module 5 for evaluating any provider apply here too.
What the Research Actually Shows
The psychedelic therapy research base has grown substantially since 2010. It's worth being honest about both what that research shows and where it still has significant limitations.
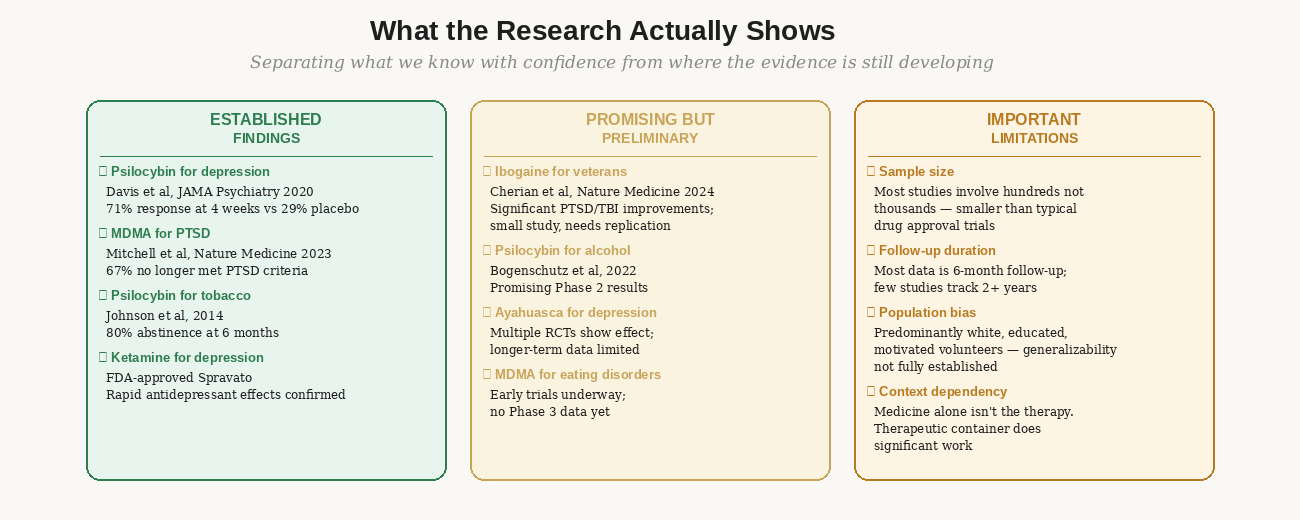
Figure 3: Separating established findings from preliminary data from genuine limitations. Both the genuine promise and the real gaps in the evidence matter for making an informed decision.
What the evidence actually establishes
The strongest evidence base is for psilocybin in depression. Davis et al (2021) in JAMA Psychiatry found a 71% response rate at four weeks in treatment-resistant depression, compared to 29% for placebo. Johns Hopkins' tobacco cessation study (Johnson et al, 2014) found 80% abstinence at six months — an extraordinary result in a notoriously treatment-resistant condition.
For MDMA in PTSD, Mitchell et al (2023) in Nature Medicine found that 67% of participants in MDMA-assisted therapy no longer met diagnostic criteria for PTSD at follow-up, versus 32% in the placebo group. The FDA's subsequent rejection of the Lykos Therapeutics application in 2024 was based on concerns about trial design and data integrity — not on evidence that MDMA doesn't work. Research continues.
For ibogaine specifically in veterans, Cherian et al (2024) in Nature Medicine found significant reductions in PTSD, depression, and anxiety symptoms in veterans with traumatic brain injuries. The study was small and needs replication, but the signal is strong enough that several programs are now specifically designed around this application.
Most studies involve hundreds of participants, not the thousands typical in pharmaceutical approval trials. Most follow-up data is at six months — very few studies track two or more years. The populations studied have been predominantly white, educated, and highly motivated volunteers. Generalizability to broader populations is not yet established.
The research is genuinely promising. It is not complete.
The Five Medicines: What Each One Does
Treating psychedelics as a monolithic category is one of the most common mistakes people make in researching this field. Psilocybin, ayahuasca, MDMA, ketamine, and ibogaine have meaningfully different mechanisms, durations, risk profiles, and what they tend to surface experientially. Choosing based on availability without understanding these differences is like choosing surgery without knowing what organ is being operated on.
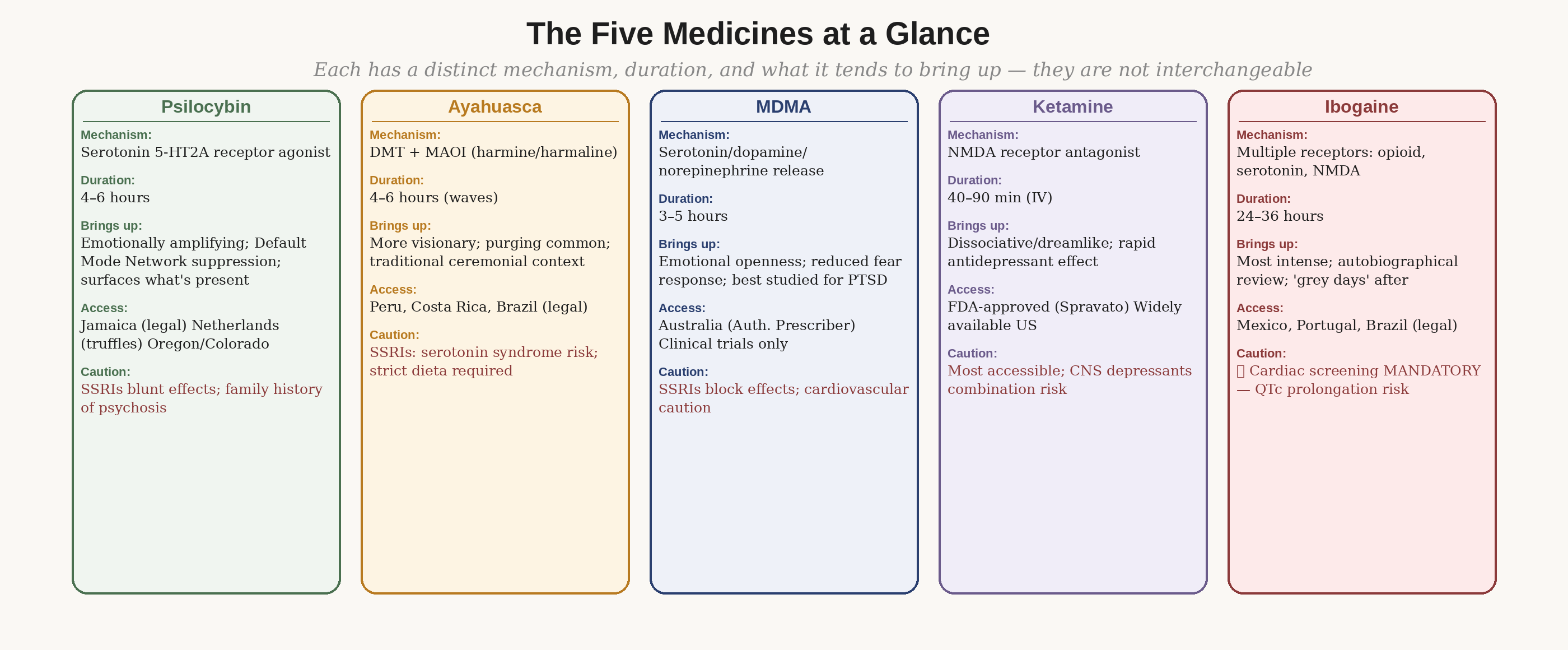
Figure 4: The five major medicines compared. Each has a distinct mechanism, duration, and what it tends to bring up. They are not interchangeable, and the preparation and contraindications differ meaningfully between them.
Psilocybin
Psilocybin is converted in the body to psilocin, which activates serotonin 5-HT2A receptors — particularly in the prefrontal cortex — producing a temporary suppression of the Default Mode Network, the brain region associated with self-referential rumination and habitual thought patterns. The experience is emotionally amplifying: whatever emotional material is present tends to surface with unusual clarity. Duration is four to six hours. The strongest evidence base of any psychedelic compound in current research.
Key caution: Contraindicated in personal or close family history of schizophrenia or psychosis. SSRIs significantly blunt effects and require tapering — Module 3 covers this in detail.
Ayahuasca
Ayahuasca is a brew combining DMT (the psychoactive compound) with MAOI alkaloids (harmine and harmaline, from the Banisteriopsis caapi vine) that allow oral DMT to be absorbed rather than broken down in the gut. The MAOI component creates the most significant drug-food and drug-drug interactions of any psychedelic. Duration is four to six hours with multiple wave peaks. Purging (vomiting) is common and considered part of the process in traditional contexts.
Key caution: The strict dietary protocol (the dieta) is pharmacological necessity, not spiritual ritual. SSRIs combined with ayahuasca carry genuine risk of serotonin syndrome. Module 3 maps the MAOI interaction profile in detail — read it before booking.
MDMA
MDMA is not a classic psychedelic in the pharmacological sense — it produces emotional openness and a dramatic reduction in fear response rather than perceptual distortion. It works primarily through massive serotonin, dopamine, and norepinephrine release. It is the most extensively studied psychedelic in clinical trials, specifically for PTSD, where its fear-reducing properties allow trauma material to be processed without the threat response that typically prevents it.
Key caution: SSRIs both block MDMA's therapeutic effects and create serotonin syndrome risk. Cardiovascular caution required. Currently accessible in clinical trials and through Australia's Authorized Prescriber pathway — not yet licensed in the US.
Ketamine
Ketamine is the most immediately accessible option in the US — FDA-approved as Spravato (esketamine nasal spray) and widely available via prescription for intravenous infusions. It works through NMDA receptor antagonism rather than serotonergic mechanisms, producing rapid antidepressant effects through a distinct pathway from classical psychedelics. The acute experience is dissociative — dreamlike, often abstract rather than emotionally narrative. Duration of the acute experience is 40–90 minutes for an infusion.
Ketamine-assisted psychotherapy — where a therapist is present during and after the infusion — produces meaningfully better long-term outcomes than infusions alone. If you're pursuing ketamine, pursue the therapy alongside it.
Ibogaine
Ibogaine carries genuine cardiac risk that categorically distinguishes it from all other medicines on this list. It prolongs the QTc interval in a way that can trigger fatal cardiac arrhythmias in people with certain underlying heart conditions — many of whom don't know they have them. Deaths have occurred at clinics that did not require cardiac screening before treatment.
Any clinic that does not require cardiac screening — ECG at minimum, ideally echocardiogram — before ibogaine treatment is operating unsafely. This is non-negotiable.
Ibogaine has produced the most striking results in addiction treatment (particularly opioid dependence) and in the emerging research on combat-related TBI and PTSD. The 2024 Stanford/Nature Medicine study showed significant improvements in PTSD, depression, and cognitive function in veterans. This is a compelling signal that warrants serious attention — and rigorous medical screening before proceeding.
Duration of ibogaine is 24–36 hours — the most demanding of all five medicines in terms of time commitment and physical intensity. The experience is often described as a forced autobiographical review. The days following (the "grey days") involve significant fatigue as the nervous system recovers. Ibogaine is legal in Mexico, Portugal, and Brazil, among other countries — it is Schedule I in the United States.
Are You Ready? An Honest Assessment
Readiness for psychedelic therapy is not a binary — it's not something you either have or don't. It's a set of conditions, some you can affect before your retreat and some you cannot. The framework below maps three zones: conditions that favor proceeding, conditions that require additional evaluation, and absolute contraindications.
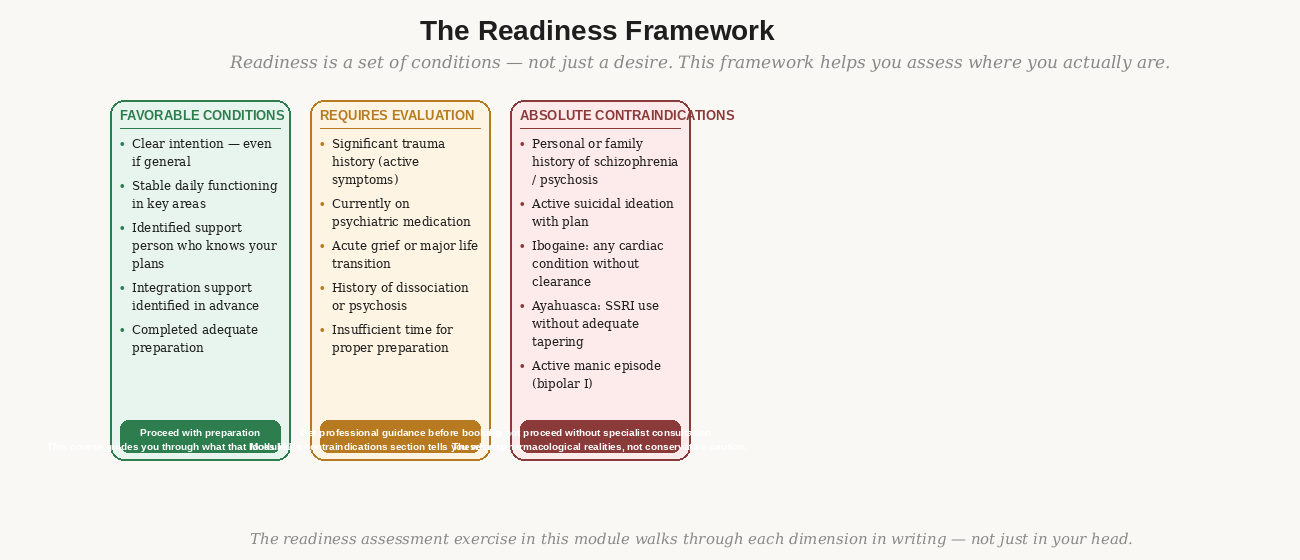
Figure 5: The readiness framework. This is not a checklist — it's a map for an honest conversation with yourself, and if needed, with a clinician. The section you're most tempted to skip is usually the most important.
A few conditions require specific emphasis because they are the most commonly underreported:
Psychiatric medication: Almost all psychiatric medications interact with psychedelic compounds in ways that range from simply reducing effects (SSRIs and psilocybin) to genuinely dangerous (SSRIs and ayahuasca, lithium and psilocybin). If you are on any psychiatric medication, you need a conversation with a prescribing clinician before proceeding — not an anonymous online forum, a clinician. Module 3 covers medication considerations in clinical detail.
History of psychosis or schizophrenia: Personal or close family history of psychosis or schizophrenia is a contraindication for classic psychedelics (psilocybin, ayahuasca). This is not conservative caution — it reflects a genuine and documented risk of psychotic episode precipitation. This applies to first-degree relatives (parents, siblings) as well as personal history.
Active suicidal ideation with plan or intent: Not passive thoughts about not wanting to be alive — active ideation with a specific plan. This requires clinical stabilization before any psychedelic intervention is appropriate.
The section people most want to skip is the contraindications — specifically, the honest self-assessment of whether now is actually the right time. There's a version of psychedelic enthusiasm that functions as bypass: a desire for something powerful enough to cut through years of difficulty without the slower work of building the conditions for genuine change.
The research on adverse outcomes consistently identifies inadequate screening and insufficient preparation as primary risk factors. The hardest thing this module asks is to sit with the possibility that now might not be the right time. Readiness is a condition, not a desire. This course will still be here when you're ready.
Personal Readiness Self-Assessment
Time required: 45 minutes minimum · Complete in writing, not just in your head
This exercise has five sections. Don't skip any of them. The section you're most tempted to skip is usually the most important one. Complete this in a dedicated journal — handwriting produces different cognitive processing than typing, and this exercise benefits from that difference.
Section A — Why Now
- What specifically is bringing you to this now — not the general reasons psychedelic therapy might be useful, but what is happening in your life that makes this feel necessary?
- How long have you been considering this? What changed recently?
- What have you already tried, and what happened with each?
- Is there any part of you pursuing this to avoid something rather than move toward something? Sit with this question for longer than is comfortable.
Section B — Current Life Stability
Rate each area 1–5 (1 = significantly unstable, 5 = solid and stable), then write one honest sentence about each:
- Daily functioning (sleep, eating, work performance): ___
- Primary relationships (partner, close family): ___
- Financial situation: ___
- Emotional baseline over the past 3 months: ___
- Support system — people who would be there if you needed: ___
Section C — Medicine and Context
- Which medicine are you considering, and specifically why that one rather than the others?
- What do you know about the program or facilitator you're considering? What have you actually verified versus what have you assumed?
- What is your primary concern about the experience? Name it specifically.
Section D — Contraindication Review
Answer honestly. These are not judgment questions — they are pharmacological realities.
- Personal or family history (first-degree relatives) of schizophrenia, psychosis, or bipolar I disorder? Yes / No
- Active suicidal ideation with intent or plan (not passive thoughts)? Yes / No
- Currently taking SSRIs, SNRIs, MAOIs, lithium, tramadol, or any antipsychotic? Yes / No
- Any cardiac condition, arrhythmia, or family history of sudden cardiac death? Yes / No — Critical if considering ibogaine
- Currently in acute grief, major loss, or significant life disruption within the past 3 months? Yes / No
- History of significant dissociative episodes? Yes / No
Section E — Integration Readiness
- Who knows you are doing this? Name them. Is there someone who will be physically present for you in the days after you return?
- Have you identified an integration therapist or coach? (Not required — but if you haven't, what is your plan for support when difficult material surfaces?)
- What does your first week after the retreat look like? Is there time protected — low demands, space to rest and reflect?
- What would you do if the experience was significantly more difficult than you expected?
Reading your answers
Read back through everything you wrote. Notice where you felt resistance. Notice which questions you answered most quickly — fast answers sometimes indicate avoidance rather than clarity. Any contraindications identified in Section D require professional consultation before proceeding. Any area of significant instability in Section B warrants honest reflection about timing.
If you're uncertain after completing this, Module 1's resources section includes organizations that can help you assess readiness with a qualified clinician.
The thing people most want to avoid in this module is the contraindications section — specifically, the honest self-assessment of whether they're actually ready.
There is a version of psychedelic enthusiasm that functions as bypass — a desire for something powerful enough to cut through years of pain without the slow work of building the conditions for genuine change. The research on adverse outcomes consistently identifies inadequate screening and preparation as primary risk factors.
The hardest thing this module asks: can you sit with the possibility that now might not be the right time? Readiness is a condition, not a desire. This course will still be here when you are.
- Can you articulate in one or two sentences what you're hoping psychedelic therapy will do for you — while genuinely holding that outcome as uncertain?
- Have you reviewed the contraindications section honestly? Is there anything there that warrants a clinical conversation before you proceed?
- Have you identified which medicine you're considering, and do you understand specifically why that one rather than the others?
- Do you have at least one person who will know you are doing this — someone who could be reached in an emergency?
- Is there any aspect of your readiness that you have been avoiding looking at directly? Name it here, even briefly.
Resources
Books
How to Change Your Mind — Michael Pollan. The most accessible overview of the contemporary psychedelic renaissance. Read critically, but excellent context for anyone new to this field.
The Body Keeps the Score — Bessel van der Kolk. Not specifically about psychedelics, but essential reading for understanding trauma — which is often the substrate psychedelic therapy works with.
Research
Davis, A.K. et al. (2021). Effects of Psilocybin-Assisted Therapy on Major Depressive Disorder: A Randomized Clinical Trial. JAMA Psychiatry, 78(5), 481–489.
Mitchell, J.M. et al. (2023). MDMA-assisted therapy for moderate to severe PTSD. Nature Medicine, 29, 2402–2415.
Cherian, K.N. et al. (2024). Magnesium-ibogaine therapy in veterans with traumatic brain injuries. Nature Medicine, 30, 373–381.
Support and evaluation
MAPS (maps.org) — The Multidisciplinary Association for Psychedelic Studies maintains a therapist directory and patient resources, including pre-session guidance.
Psychedelic Support (psychedelic.support) — Directory of integration therapists with specific psychedelic training, searchable by location.
Fireside Project (firesideproject.org) — 24/7 psychedelic peer support line. Call or text 62-FIRESIDE. Relevant both before and after your session.