Physical Preparation — The Body Is Not Optional
- Understand why physical preparation is pharmacologically significant — not a wellness ritual but a direct determinant of safety and experience quality.
- Know the specific dietary and substance restrictions for each of the five major medicines, including the pharmacological reason each restriction exists.
- Have a clear framework for handling the medication question — including what to ask your doctor and why self-tapering is dangerous regardless of your circumstances.
- Have completed the 8-week preparation timeline and adapted it to your specific medicine and retreat date.
- Know what to eat and avoid on the day of your session, and what physical state you're aiming to arrive in.
Opening
Most preparation guides talk about the body last — as if dietary adjustments and medication review are administrative details to be handled after the real work of intention-setting and emotional preparation. This is backwards. The body is the vessel through which the experience occurs. What you put into it in the weeks before — and what you remove — has direct pharmacological consequences that can mean the difference between a productive experience and a dangerous one.
This is especially true for ayahuasca, where the MAOI component of the brew creates genuine drug-food and drug-drug interactions that are not cautionary suggestions. They are pharmacological facts. Eating aged cheese within 24 hours of an ayahuasca ceremony while on an SSRI is not a minor risk factor — it is a combination that can trigger serotonin syndrome or hypertensive crisis, both of which can be fatal. A good retreat center will screen for this. A poor one won't. You need to know this regardless.
But physical preparation matters even when the risks are less acute. Arriving at a retreat after a week of poor sleep, alcohol, and stress is arriving with a compromised nervous system. The experience will still occur — but the quality of what's possible is directly related to the quality of the container you bring to it. A calm, rested, nourished nervous system creates different conditions than a depleted one.
This module is the most practically specific in the course. Work through it carefully. Use the timeline. Talk to your doctor. Do not skip the medication section even if you think it doesn't apply to you — the most dangerous interactions are often from medications people don't think of as psychiatric.
Why Physical Preparation Matters Pharmacologically
The distinction between pharmacological and experiential preparation matters because it affects how seriously you take it. If preparation is a spiritual practice — a ritual of purification — then it's something you can modify based on how you feel. If preparation is pharmacological — something that directly affects how the compound interacts with your body — then it isn't optional.
For some medicines, particularly ayahuasca and ibogaine, physical preparation is a safety matter. For all medicines, it is an experience-quality matter. Here's the mechanism:
Pharmacological window
Psychedelic compounds interact with receptor systems that are already occupied by medications, foods, and other substances. SSRIs, for example, occupy 5-HT2A serotonin receptors — the same receptors that psilocybin activates. When those receptors are already occupied, psilocybin's effects are significantly blunted, and the interaction becomes pharmacologically unpredictable. Removing competing substances allows the medicine to work as studied.
Nervous system state
Alcohol is a CNS depressant. Chronic cannabis use creates a blunted endocannabinoid system. High caffeine intake creates baseline cortisol elevation and anxiety. Chronic sleep deprivation activates stress-response pathways. Each of these creates a baseline physiological state that the medicine then amplifies. Reducing them in the weeks before arrival doesn't just follow a wellness protocol — it changes the physiological starting point.
Hepatic load
Many psychedelic compounds, including ayahuasca and ibogaine, are metabolized by the liver. Alcohol, many medications, and some supplements compete for the same metabolic pathways. Reducing the liver's burden in the weeks before a session allows the medicine to be metabolized more cleanly and predictably.
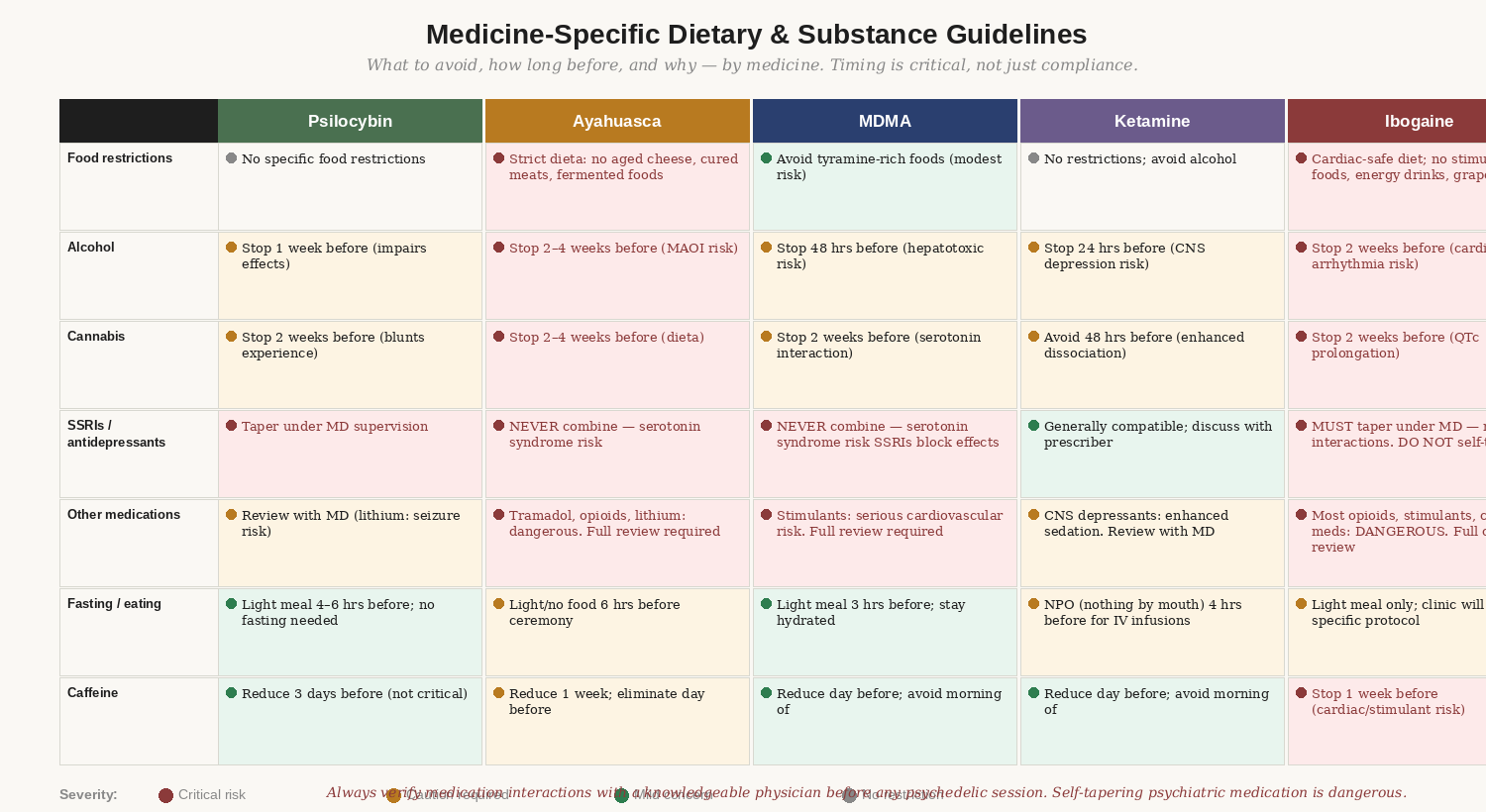
Figure 1: What to avoid and for how long before each medicine. These are pharmacological requirements, not suggestions.
The Five Pillars of Physical Preparation
Pillar 1: Medication Review
This is the most important and most frequently skipped part of physical preparation. Medication interactions with psychedelic compounds range from reducing efficacy to creating life-threatening emergencies. The general rule: if you are taking any medication regularly — psychiatric, cardiovascular, pain, or otherwise — you need a physician review before your session, ideally with a doctor who understands psychedelic medicine.
The challenge is that most general practitioners don't know the interaction profiles of psychedelic compounds, because these are not conventionally prescribed medications. If your GP isn't familiar, you have two options: educate them (bring the relevant pharmacology — see the Resources section at the end of this module) or find a knowledgeable integrative physician through MAPS or Psychedelic Support.
We'll cover medication-specific guidance in the next section. The key point here: do not self-taper, and do not assume that medication review is only necessary for people with complex psychiatric histories. Common medications — tramadol, prescribed for pain; certain antibiotics; St. John's Wort — carry significant interaction risks that most people wouldn't think to raise.
Pillar 2: Diet and Substance
Dietary restrictions exist for pharmacological reasons, not spiritual ones — though the traditional framing of the dieta in Amazonian plant medicine cultures captures something real about the relationship between what you consume and what you can perceive. For ayahuasca, the restrictions are medically significant. For other medicines, they are primarily about arriving with a clean physiological baseline.
The most important substances to reduce across all medicines: alcohol (minimum one week before, preferably two to four), cannabis (minimum two weeks before — the endocannabinoid system takes longer to recalibrate than most people realize), recreational stimulants, and heavy processed food loads. These aren't purity requirements — they're practical pharmacology.
Pillar 3: Sleep and Recovery
Sleep deprivation is the single most reliable predictor of a difficult psychedelic experience in people who don't have other obvious risk factors. This is not superstition — it is basic neuroscience. The prefrontal cortex, which helps regulate emotional responses and supports top-down control during challenging experiences, is the brain region most affected by sleep deprivation. Arriving sleep-deprived means arriving with compromised capacity to work with difficult material.
The goal in the two weeks before a retreat is consistent sleep — seven to nine hours nightly, with a consistent sleep and wake time. Reducing screen time in the hour before bed, avoiding alcohol (which disrupts REM sleep even in small amounts), and managing stress levels all contribute to sleep quality. If you have a chronic sleep condition, this is worth raising with your preparation therapist or facilitator.
Pillar 4: Movement and Stress
Regular gentle movement in the weeks before your retreat supports the nervous system in two ways: it creates regular discharge of accumulated physical tension (important if you carry chronic stress or trauma in the body, as most people do), and it primes the body for the physical demands of the session. Psychedelic sessions are physically demanding — lying still for six to eight hours, moving through intense emotional states, processing in the body — in ways that are easy to underestimate from the outside.
The caveat: very high-intensity exercise in the days immediately before a session can leave you physically fatigued and create elevated cortisol, which works against you. Wind down to gentle movement — walking, yoga, swimming — in the week before. Your body needs to arrive rested, not depleted.
Pillar 5: Session Day Preparation
The day of your session has its own specific preparation requirements, which vary by medicine. The general principle: arrive physically comfortable, not full, not hungry, hydrated, and as rested as possible. The specific requirements will be covered in the medicine-specific section below.
Medicine-Specific Dietary and Substance Guidelines
The following applies across all medicines: stop all recreational drugs at least two weeks before your session. This includes cannabis, even if medically prescribed. If you are in a medical cannabis program for a condition, discuss this specifically with your facilitator and physician — for some conditions, the calculus is different, but the default assumption should be discontinuation.
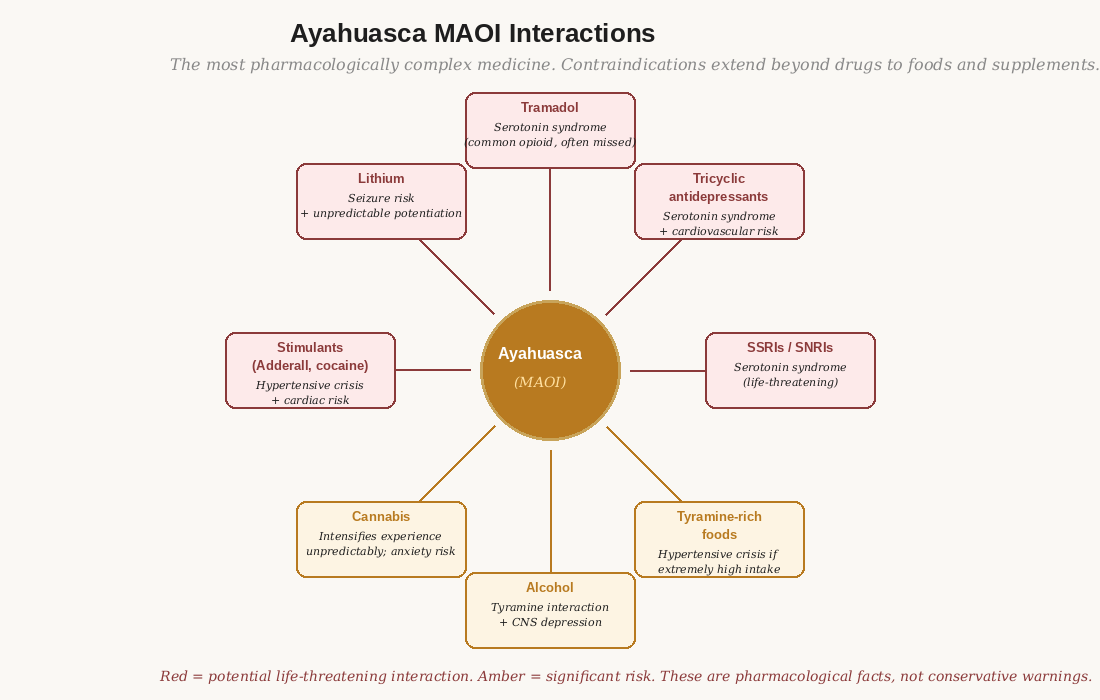
Figure 2: The ayahuasca MAOI interaction map. The dieta is pharmacological necessity, not spiritual ritual.
Psilocybin: The Most Forgiving Profile
Psilocybin has the most permissive dietary profile of the five major medicines. There are no specific food restrictions with significant pharmacological basis. The most important dietary consideration is what you eat on the day of the session: a light meal four to six hours before (not fasting completely, as low blood sugar during the experience creates physical discomfort; not a full meal, as nausea is more likely with a full stomach).
The significant medication concern is SSRIs and SNRIs. These occupy the 5-HT2A receptors that psilocybin activates. In most cases, SSRIs significantly blunt the psilocybin experience. Whether this is a reason to taper depends on your psychiatric stability and how important full-dose effects are to your therapeutic goals. This should be a conversation with your prescribing physician. Abrupt SSRI discontinuation carries its own risks — particularly discontinuation syndrome, which can include intense mood instability. The most common SSRI discontinuation protocols call for two to four weeks of gradual reduction; fluoxetine (Prozac) has a five-week half-life and requires a longer taper than other SSRIs.
Ayahuasca: The Most Complex Profile
The dieta is not optional. It is pharmacology.
Ayahuasca contains harmala alkaloids (harmine, harmaline, tetrahydroharmine) that reversibly inhibit monoamine oxidase A (MAO-A). MAO-A normally breaks down monoamine neurotransmitters — serotonin, dopamine, norepinephrine — and dietary tyramine. When MAO-A is inhibited, these substances accumulate to levels that can cause life-threatening effects.
Serotonin syndrome: SSRIs + ayahuasca MAOI → serotonin accumulates → agitation, hyperthermia, rapid heart rate, muscle rigidity, seizures. Can be fatal.
Hypertensive crisis: high-tyramine foods + ayahuasca MAOI → tyramine accumulates → sudden severe hypertension. Can be fatal.
These are not theoretical risks. Both have occurred in retreat settings.
The traditional ayahuasca dieta restricts aged and fermented foods (aged cheeses, cured and fermented meats, fermented soy products such as miso and soy sauce, sauerkraut and kimchi, overripe or dried fruit), alcohol, pork, and recreational drugs. These restrictions should begin two to four weeks before ceremony and be maintained until at least 24 hours after.
The medication list for ayahuasca is extensive. SSRIs and SNRIs are absolute contraindications without adequate tapering. Tramadol — a common prescription pain medication that inhibits serotonin reuptake — carries serotonin syndrome risk. Lithium should not be combined with any classic psychedelic due to seizure risk. If you are on any psychiatric medication and considering ayahuasca, you need a physician review before booking. A responsible retreat center will ask about this in their screening. If they don't, that is a warning sign.
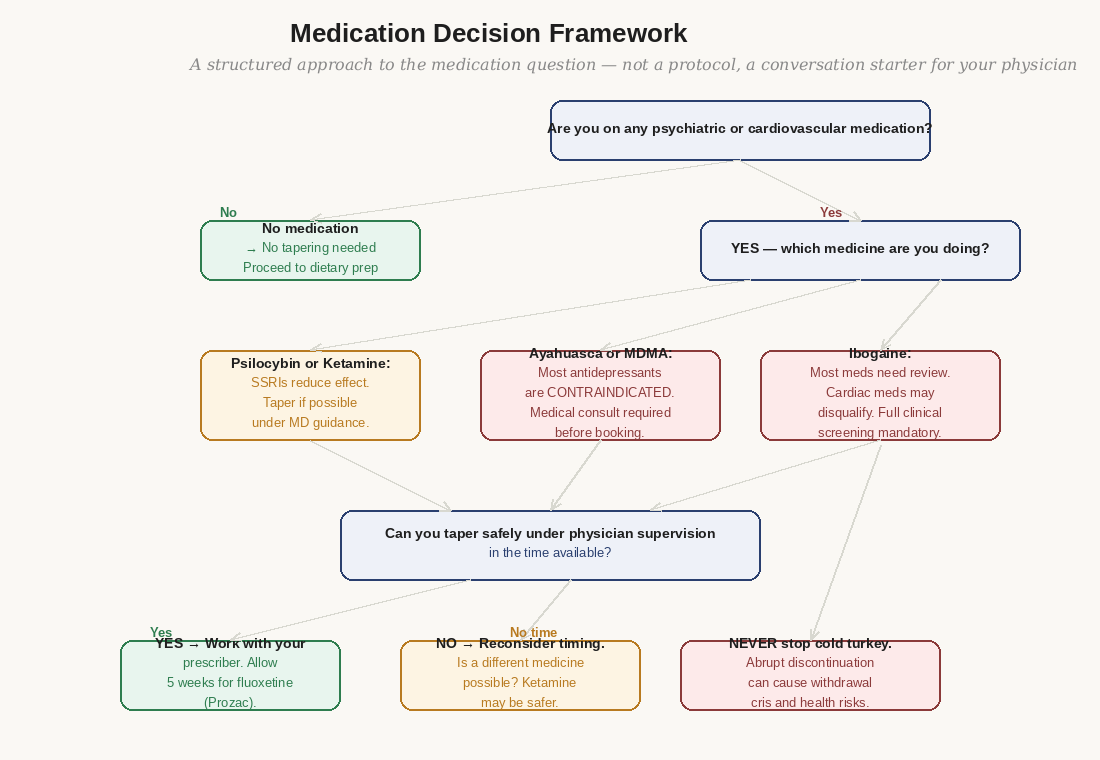
Figure 3: How to approach the medication question — what requires stopping, tapering, specialist guidance, or is an absolute contraindication.
MDMA: Cardiovascular and Serotonergic Concerns
MDMA carries two primary physical preparation concerns: serotonergic interactions and cardiovascular demands. Like ayahuasca, MDMA should never be combined with SSRIs — the combination creates serotonin syndrome risk and, paradoxically, SSRIs block MDMA's effects by competing for the same transporter proteins. The combination is both dangerous and counterproductive.
MDMA creates cardiovascular demands — it elevates heart rate and blood pressure during the session. If you have cardiovascular disease, uncontrolled hypertension, or a history of cardiac arrhythmia, MDMA is contraindicated. A physician review is necessary if you have any cardiovascular history.
Dietary restrictions for MDMA are less strict than for ayahuasca — there is no MAOI mechanism creating tyramine risks. The most important physical preparation points are adequate hydration (hyponatremia — dangerously low sodium from overdrinking — has occurred when people drink excessive water during MDMA sessions; maintain normal hydration, not excessive), and adequate rest before and after.
Ketamine: The Most Medically Supervised Profile
Ketamine is administered in clinical settings in the US, which means the physical preparation requirements are managed by the clinical team. For IV ketamine infusions, the standard protocol is NPO — nothing by mouth, including water — for four hours before the procedure. This is standard pre-procedure practice to reduce aspiration risk during sedation.
The most significant medication interaction concern with ketamine is other CNS depressants — benzodiazepines, opioids, alcohol — which can potentiate sedation to dangerous levels. If you are on any of these medications, your prescribing clinician will manage this. The other concern is dissociative medications, including some antipsychotics, which can interact unpredictably.
For Spravato (intranasal esketamine), the clinical protocol manages most of these considerations. Your treatment team will review your medications before each session. For IV ketamine at a ketamine infusion center, the quality of the screening varies — a center that doesn't review your full medication list before infusion is not operating safely.
Ibogaine: The Highest Physical Risk Profile
Ibogaine requires cardiac clearance before any treatment. This is non-negotiable.
Ibogaine prolongs the QTc interval — the electrical interval measured on an ECG that governs cardiac rhythm. QTc prolongation can trigger fatal arrhythmias (ventricular fibrillation, torsades de pointes) in people with certain cardiac risk factors. Deaths have occurred at ibogaine clinics that did not perform cardiac screening. The risk is not rare.
Minimum cardiac screening: a 12-lead ECG reviewed by a physician who knows ibogaine. More thorough screening includes bloodwork (electrolytes, liver function), a thorough cardiac history, and for people over 40 or with cardiac risk factors, a cardiologist consultation.
If a clinic does not require cardiac screening before treatment — walk away.
Beyond cardiac clearance, ibogaine's complex pharmacology creates interactions with a wide range of medications. Most opioids must be tapered before ibogaine — there are specific ibogaine-opioid interaction risks depending on the opioid. Stimulants are contraindicated. Methadone and buprenorphine require specific protocols before ibogaine, because these medications have long half-lives and complex interactions with ibogaine's mechanism.
The physical experience of ibogaine is demanding in a way that the other medicines are not. The experience lasts 24–36 hours. The first 8–12 hours are often intensely visual and internally confrontational. This is followed by the 'gray days' — a period of lowered mood, fatigue, and sensitivity lasting two to four days. Arriving physically depleted or unwell will significantly worsen this period. Rest, nutrition, and physical preparation matter for ibogaine more than any other medicine.
The Medication Question: A Framework
The medication question is where most people either skip (assuming it doesn't apply to them) or become paralyzed (unsure how to navigate a conversation their GP doesn't know how to have). Here is a framework for approaching it.
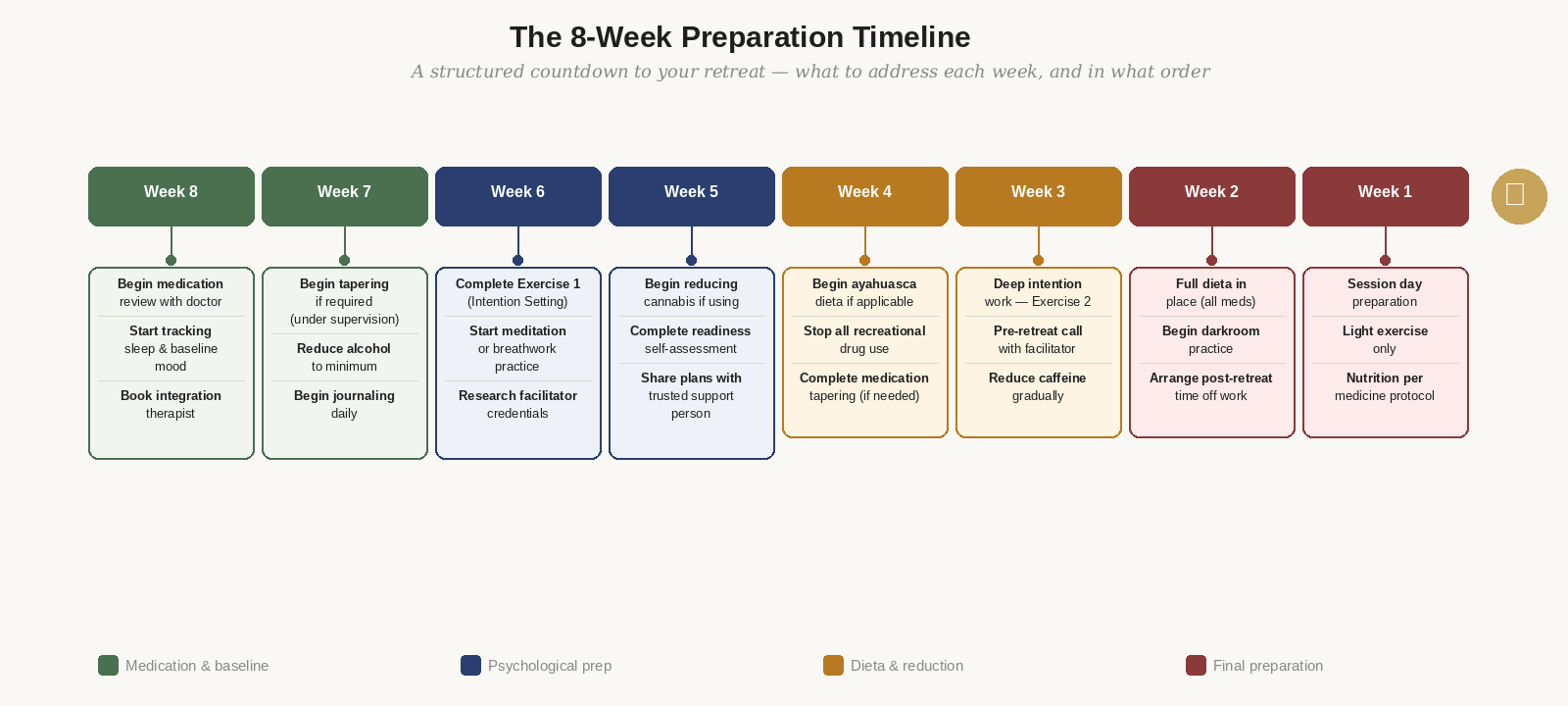
Figure 4: Week-by-week schedule from eight weeks before through the session day.
Who needs a physician review
Everyone who is currently taking any prescription medication — not just psychiatric medications. The list of unexpected interactions is long. Common surprises: tramadol (opioid pain medication with serotonin reuptake inhibition), certain antibiotics (some have QTc effects relevant to ibogaine), St. John's Wort (MAOI properties — dangerous with ayahuasca), some antihistamines (anticholinergic effects), and certain supplements including 5-HTP and L-tryptophan (serotonin precursors, risky with MDMA and ayahuasca).
How to have the conversation
Your GP may not know the pharmacology of these compounds. This is not a failure — it's a consequence of these medicines not being part of conventional medical training. You can help by bringing specific information. A good approach: 'I'm planning to attend a therapeutic retreat involving [medicine]. I want to make sure my current medications don't create interactions. Here are the specific interaction concerns I've researched — can we review my medications against these?'
Bring a printed list of known interactions for your specific medicine. MAPS maintains publicly available pharmacology sheets for MDMA-specific interactions. For ayahuasca, the Erowid Vault has a comprehensive MAOI interaction database. For ibogaine, Multidisciplinary Association for Psychedelic Studies and the Global Ibogaine Therapy Alliance maintain safety resources.
What 'tapering' actually means
Tapering is the gradual reduction of a medication's dose over time, rather than stopping abruptly. The purpose is to allow the body to adjust to lower levels, reducing withdrawal effects. For SSRIs, the standard approach is reducing dose by 10–25% every two to four weeks. This is slower than many physicians routinely recommend — but rapid tapering increases discontinuation syndrome symptoms.
The critical point: tapering should never be done on your own timeline without medical supervision. If your doctor recommends a faster taper than this, discuss the rationale. If you are tapering because of retreat plans, be explicit about the timeline — your doctor needs to know the endpoint date. And factor in the medication's half-life: fluoxetine (Prozac) has a five-week half-life, meaning it stays in your system weeks after you stop taking it, and requires a longer preparation window than other SSRIs.
When there isn't enough time
Sometimes the honest answer is: you've left yourself insufficient time to safely taper and complete preparation for the medicine you want to do. This is more common than people expect. The appropriate response is not to proceed anyway — it is to either reschedule to allow adequate time, or to consider whether a different medicine (typically ketamine, which has the most permissive medication profile) is a better fit for your current situation.
What to Eat and Avoid — The Day Of
General principles across all medicines:
- Eat a light meal four to six hours before the session. Not fasting — low blood sugar creates physical discomfort that adds to the challenge of an already demanding experience. Not a full meal — a full stomach increases nausea and gastric discomfort.
- Stay well hydrated during the day. Reduce fluid intake in the two hours immediately before to minimize the need for bathroom interruptions early in the session.
- Avoid caffeine on the day of. Caffeine creates baseline anxiety and cortisol elevation that works against the experience.
- Avoid alcohol completely for at least 24 hours before. The night before a session is not the time for 'one drink to calm your nerves.'
Medicine-specific additions:
- Ayahuasca: Continue the strict dieta on the day of ceremony. The maloca typically begins at 8pm — a light, tyramine-free meal before 2pm is appropriate. No food after that.
- Psilocybin: Light meal four to six hours before. Some facilitators suggest ginger tea if nausea is a concern — ginger has mild anti-nausea properties that don't interfere with the session.
- MDMA: Light meal three hours before. Important: maintain normal hydration — not excessive water intake. Hyponatremia is a real risk with MDMA and results from overdrinking, not underdrinking.
- Ketamine (IV): NPO four hours before as instructed by clinical team. Follow clinical instructions precisely.
- Ibogaine: Follow clinic-specific protocol. Most ibogaine clinics have detailed pre-session nutrition guidelines. Follow them precisely.
The thing people most want to avoid in this module is the medication conversation with their doctor.
There are several reasons people avoid it: they fear their doctor will try to talk them out of it; they don't want to admit they're planning something outside mainstream medicine; they assume their medications are fine without checking; or they've left themselves insufficient time for tapering and don't want to face that fact.
Each of these reasons has produced harm. People have attended ayahuasca retreats on SSRIs without disclosing their medications, experienced serotonin syndrome, and required emergency medical intervention. People have attended ibogaine clinics without cardiac clearance and died. These are not abstractions — they are documented events.
Your doctor's job is your physical safety. Whatever their personal view on psychedelic therapy — and many physicians are now well-informed and supportive — they need accurate information about your plans to do their job. Give it to them.
If your doctor is dismissive or uninformed, find a more knowledgeable one for this specific consultation. You don't have to switch primary care providers — you need one informed consultation. MAPS, Psychedelic Support, and the Society of Psychedelic Practitioners maintain referral lists.
Exercise: The 8-Week Preparation Timeline
Time required: 30 minutes to complete the initial plan; ongoing over 8 weeks.
Materials: A calendar (digital or paper) and a printed or digital copy of this timeline.
Important: Complete this exercise immediately after reading this module, while the specific guidance is fresh. A plan that stays in your head is not a plan.
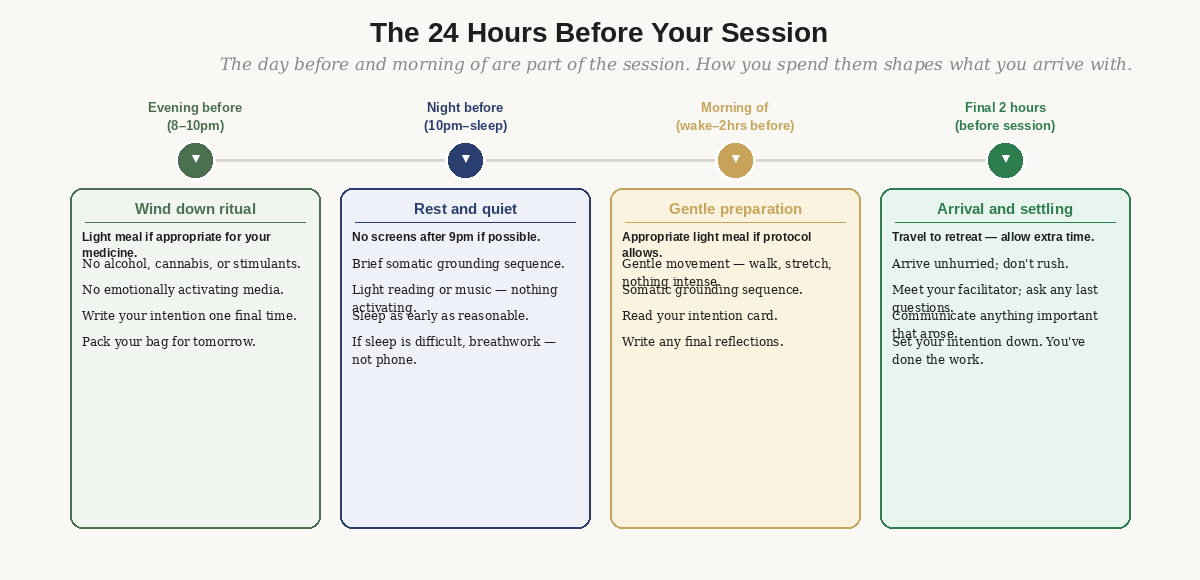
Figure 5: The final 24 hours — what to do and avoid physically, emotionally, and practically.
Step 1: Anchor the timeline to your retreat date
Write your retreat date at the top of a blank page or calendar. Count backward and mark each week — Week 8, Week 7, down to Week 1 (the final week before your retreat).
Step 2: Schedule non-negotiable milestones first
These have fixed lead times that cannot be compressed. Schedule them before anything else:
- Physician consultation for medication review — schedule this for Week 8, as soon as possible. If tapering is required, you need the full eight weeks.
- Contact your facilitator or retreat center — Week 7 or 8. Request a pre-retreat preparation call. Ask specifically about their medication screening requirements.
- Identify and contact an integration therapist — Week 7. You want this relationship in place before your retreat, not after.
- Arrange post-retreat time off work — Week 6. You need at least three days, ideally five, with no significant demands. This is not a recovery period from an illness; it is a neurologically active integration window that requires quiet.
Step 3: Set reduction milestones for substances
Working backward from your retreat date, mark:
- Alcohol: last drink [date = retreat date minus 14 days minimum; ayahuasca minus 28 days]
- Cannabis: last use [date = retreat date minus 14 days minimum]
- Caffeine: begin reduction [date = retreat date minus 21 days]; eliminate [date = retreat date minus 7 days]
- If applicable — begin dieta [date depends on medicine and retreat center guidance]
Step 4: Schedule your preparation practices
Mark these on your calendar as recurring appointments, not intentions:
- Daily journaling: begins [Week 8] — 15 minutes each morning
- Meditation or breathwork practice: begins [Week 7] — even 10 minutes daily builds significant capacity
- Complete Exercise 1 (Intention Setting): [Week 6]
- Complete Exercise 2 (Readiness Reflection): [Week 5]
- Pre-retreat call with facilitator: [Week 3]
- Arrange post-retreat support contact: [Week 2]
Step 5: Write the day-before and day-of protocols
On a separate card or page, write specifically:
- What you will eat the day before (light, medicine-appropriate)
- What time you will eat the day of, and what
- What you will do the morning of (gentle movement, quiet time, reading your intention)
- What you will bring to the retreat (comfort item, journal, eye shades, water)
- Who knows you are going and how to reach you in an emergency
Keep this card somewhere you'll see it in the final week. The preparation period should reduce anxiety, not amplify it. If you find that completing this timeline is generating significant anxiety, bring that to your pre-retreat call with your facilitator — this is exactly what that call is for.
- Have you scheduled a physician consultation for medication review? If any of your medications appear on the interaction lists for your specific medicine, has this been discussed with your doctor?
- Do you have a written 8-week preparation timeline with specific dates? Is it in your calendar?
- Have you identified your dieta start date and what the restrictions are for your specific medicine?
- Do you know what you will eat on the day of the session, and approximately when?
- Is there any part of the physical preparation you've been avoiding or minimizing? Name it — and decide what you're going to do about it.
Resources
Medical References
Ruffell, S. et al. (2020). The pharmacological interaction of compounds in ayahuasca: a systematic review. Revista Brasileira de Psiquiatria, 42(6), 646–656. The most comprehensive review of ayahuasca drug interactions — useful reference to share with your physician.
Cherian, K.N. et al. (2024). Magnesium-ibogaine therapy in veterans with traumatic brain injuries. Nature Medicine. Includes the cardiac monitoring protocol used at Ambio Life Sciences — a useful reference for understanding ibogaine screening standards.
Practical Tools
MAPS MDMA Therapy Participant Information (maps.org) — includes preparation and contraindication materials developed for Phase 3 clinical trials. Detailed medication interaction guidance.
Erowid MAOI Combination Chart (erowid.org/chemicals/maois/maois_combination.shtml) — comprehensive database of MAOI interactions, including foods and supplements. Essential reference for anyone considering ayahuasca.
Global Ibogaine Therapy Alliance — GITA Safety Guidelines (available at ibogainealliance.org) — the field-standard safety protocol for ibogaine treatment including cardiac screening requirements.
Finding a Knowledgeable Physician
Society of Psychedelic Practitioners (psychedelicpractitioners.org) — Directory of physicians and mental health professionals with psychedelic medicine training. Useful for finding a knowledgeable physician for the medication consultation.
Psychedelic Support directory (psychedelic.support) — Includes physicians and nurse practitioners with psychedelic medicine training who can advise on medication questions.