Set and Setting — The Two Variables That Matter Most
- Understand the clinical evidence for why set and setting account for more outcome variance than the compound itself — and what that means practically.
- Know how to evaluate a facilitator or retreat center using specific, concrete criteria — and what the red flags are that most people miss until too late.
- Understand the meaningful differences between ceremonial maloca settings, Western therapeutic retreats, licensed service centers, and clinical trials — and which suits your situation.
- Have a detailed plan for the 24 hours before your session, including what to do and what to avoid, based on your specific medicine.
- Have completed the pre-session facilitator conversation guide so you can communicate your history and intention effectively in a ten-minute intake call.
Opening
Timothy Leary's original formulation of "set and setting" in the 1960s was an attempt to explain why the same dose of the same compound could produce ecstatic insight in one person and a terrifying crisis in another. The answer, he argued, was not primarily in the molecule — it was in the mindset the person brought (set) and the environment in which the experience occurred (setting). Fifty years of research has refined but not refuted this observation. Modern psychedelic science consistently finds that set and setting account for significantly more variance in outcomes than dose alone.
This is both encouraging and sobering. Encouraging because it means that much of what determines your experience is within your influence — you can shape your mindset, you can choose your setting carefully, you can build a relationship with your facilitator before the session. Sobering because it means that the experience is not simply a function of taking the medicine. Arriving unprepared, in a poorly facilitated setting, without having done the work of the previous four modules — this produces different results than arriving prepared, in a skilled setting, with a clear intention and a regulated nervous system.
This module covers the practical decisions that set and setting require: how to choose and evaluate a program, how to choose between formats, how to prepare the setting within your control, and how to use the final 24 hours before your session. Many of these decisions have already been made if you've booked a program. Read this module as a way of understanding what you've chosen and how to get the most from it — and as a reference for future decisions if this becomes an ongoing practice.
One of the most common preparation mistakes: spending extensive time on inner work — intention, emotional preparation, somatic practice — and almost no time on the practical questions of who is going to be in the room with you and what that room looks like. Both matter. The quality of the container that holds the experience is as important as the quality of the experience itself.
What Set and Setting Actually Mean
The terms are often used casually in psychedelic culture without much precision. It's worth being specific, because the specificity reveals what you can actually do with the concept.
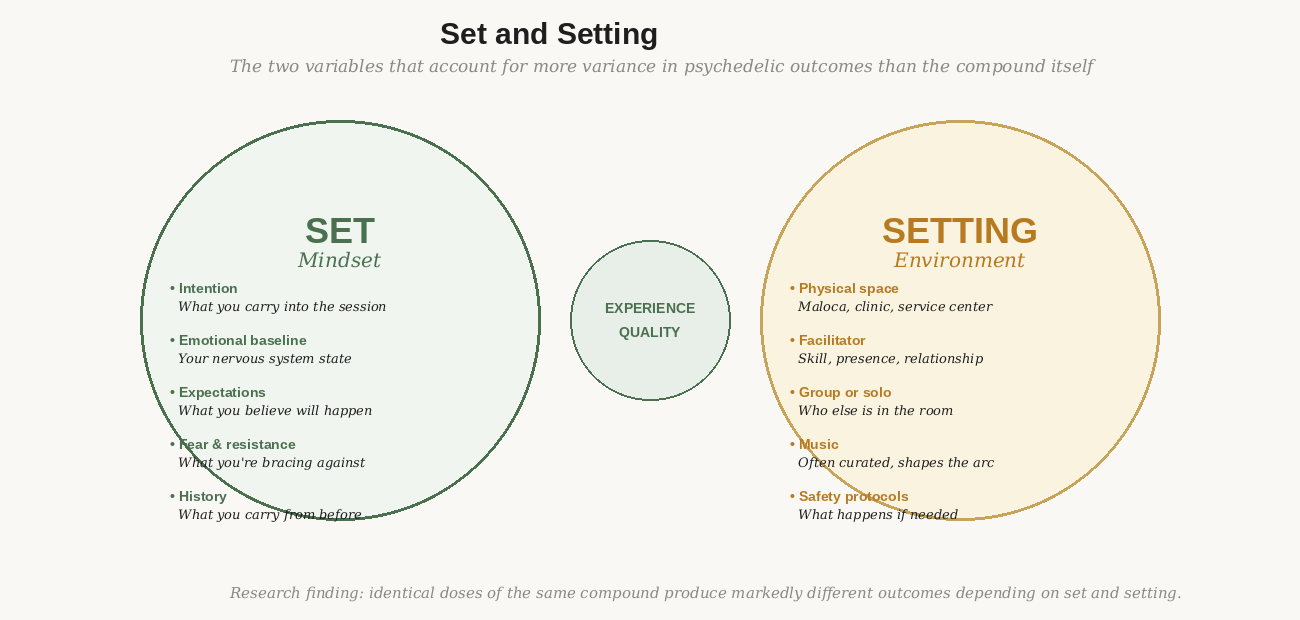
Figure 1: Set and setting account for more outcome variance than dose or compound. A well-prepared person in a poor setting typically fares worse than a moderately prepared person in an excellent one.
Set: Everything you bring to the threshold
Set is the sum of everything internal: your intention (Module 2), your emotional and nervous system state at the time of the session (Module 4), your expectations about what will happen, your fear and resistance, your relationship to uncertainty, and the specific psychological history you carry. Set is what Module 1 through 4 have been building. It is, in a real sense, everything this course has been working on so far.
The practical implication: set is not fixed on the day of your session. It has been shaped by everything you've done — or not done — in preparation. A person who has spent six weeks doing the preparation work in this course arrives with a different set than someone who spent six weeks reading trip reports. Both will have experiences. They will tend to have meaningfully different experiences.
Setting: The container that holds the experience
Setting is everything external: the physical space, the people in it (primarily the facilitator, and any co-participants in a group format), the music or soundscape, the protocols in place if something goes wrong, the quality of the facilitation. Setting is largely chosen before the session rather than created during it — this is why program selection matters enormously, and why it deserves the careful attention this module gives it.
A useful frame: setting is the container. The experience is what fills it. A strong, well-held container allows the contents to be whatever they are — including difficult — without the container failing. A weak container puts the experience at risk of becoming overwhelming not because the content is unmanageable but because the support structure is inadequate. Choosing a setting is choosing the quality of the container that will hold whatever arises.
The Research on Set and Setting
The most rigorous modern evidence for set and setting comes from several converging sources. The 2018 Johns Hopkins study on psilocybin for depression found that the magnitude of the "mystical experience" — a measure of how profoundly meaningful and ego-dissolving the experience was — was a stronger predictor of antidepressant outcomes than dose alone. Mystical experience quality is heavily shaped by set and setting.
The MAPS MDMA trials control for set and setting so thoroughly — standardized music, two trained therapists, extended preparation and integration — that some researchers have questioned whether the control condition (placebo with the same therapeutic container) is actually controlling for the right variable. This debate is ongoing. What it reveals is that the therapeutic container is doing significant work even in the absence of the active compound.
Perhaps the most striking evidence: a 1962 study by Pahnke gave high-dose psilocybin to a group of theologians in a church setting (the "Good Friday Experiment") and found profound mystical experiences. The same dose given to medical students in a clinical laboratory produced significantly different experiences. Same compound, same dose, different set and setting — meaningfully different results.
The practical implication of the research:
You cannot compensate for a poor setting with a large dose. You cannot compensate for a poor set with an excellent setting. These variables interact and multiply rather than substitute for each other. The best outcomes consistently come from the combination of thorough preparation (set) and skilled, safe facilitation (setting).
Evaluating Your Facilitator
The facilitator relationship is the single most important setting variable. More important than the physical space, more important than the music, more important than whether the venue has ocean views. The person responsible for your safety and support during one of the most significant experiences of your adult life deserves careful evaluation.
Most people do not evaluate their facilitator carefully enough. They read the retreat center's website, look at the photos, read a few testimonials, and book. This is the equivalent of choosing a surgeon based on their clinic's aesthetics. The questions below are designed to help you understand who you're actually working with.
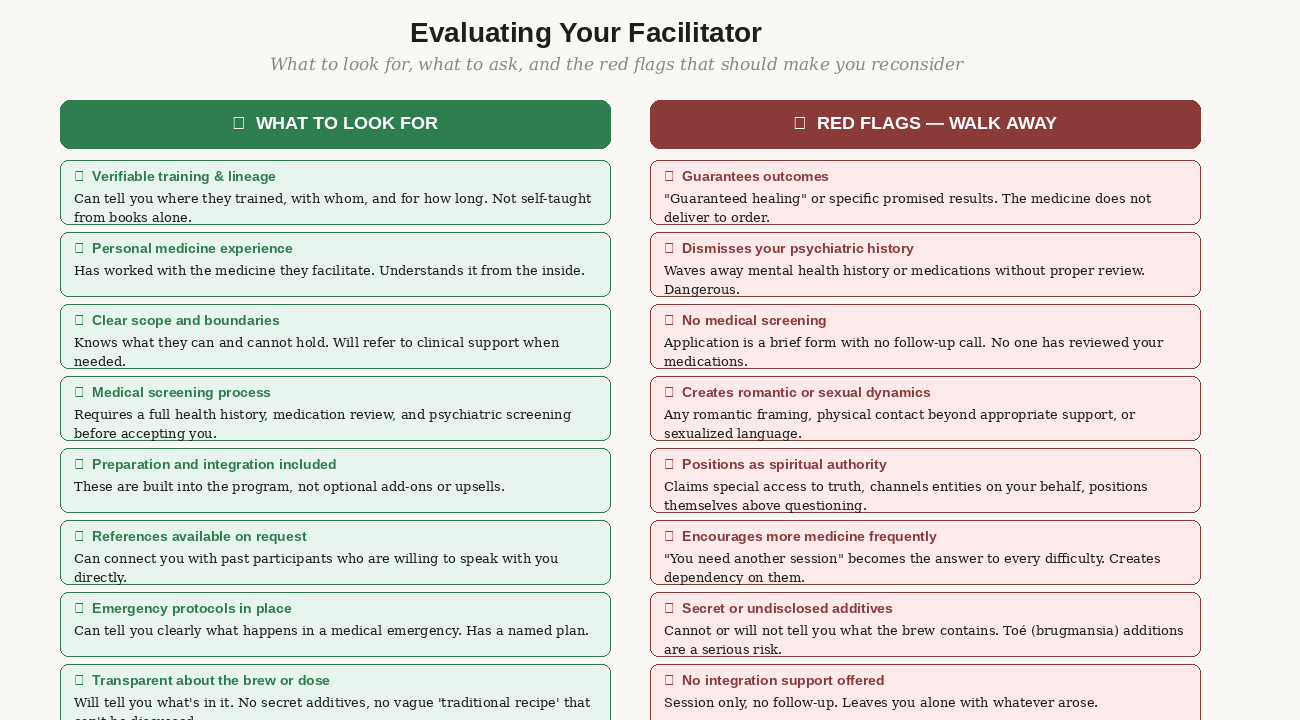
Figure 2: A 20-point evaluation framework — what to ask, what answers should look like, and the red flags that disqualify a program regardless of other qualities.
Questions to ask before you book
Most retreat centers and facilitators offer a pre-booking discovery call. Use it. These questions will tell you quickly whether someone has genuine depth or is a generalist who has added psychedelic facilitation to their offering:
- What is your training background, and with whom did you train? How long did that training take?
- Do you have personal experience with the medicine you facilitate? How has that shaped your facilitation approach?
- How do you handle a participant who becomes overwhelmed or needs support during the session? What does that look like specifically?
- What happens if someone has a medical emergency during the session? Is there a physician on site or on call?
- What does your screening process look like? Will anyone review my medications before I arrive?
- What integration support is included, and what does a typical integration circle look like?
- Can you connect me with a past participant who has similar experience to mine and is willing to speak with me?
Notice what the answers reveal. A facilitator with genuine depth will answer these questions specifically and without defensiveness. They will have clear protocols. They will be able to tell you exactly what they do when someone has a difficult experience. Vague or reassuring-but-unspecific answers to operational questions are concerning.
The facilitator relationship before the session
In the most rigorous psychedelic therapy programs — the MAPS MDMA trials, the Johns Hopkins protocols — significant time is invested in building the therapeutic relationship before any medicine is administered. Multiple preparation sessions, getting to know the therapist team, establishing trust. This is not a luxury — it is part of the therapeutic mechanism. The relationship itself creates the safety that allows difficult material to arise and be worked with.
Most retreat programs don't have the resources for multiple preparation sessions. What they can offer — and what you should expect at minimum — is a substantive pre-retreat call with your specific facilitator (not just an intake coordinator). Use this call not just to provide information but to assess the relationship. Do you feel genuinely heard? Does the facilitator ask about what you're carrying, or do they give a standard information script? Do they create the experience of being safe to be honest?
If, after a pre-retreat call, you do not have a basic sense of trust in your facilitator — if something feels off, if you felt dismissed or unheard — this matters. You can raise your concerns explicitly. You can request a different facilitator if the program allows. You can reconsider the program. Going in without basic trust in the person responsible for your safety is a significant set-and-setting liability.
Setting Formats: What Each One Offers
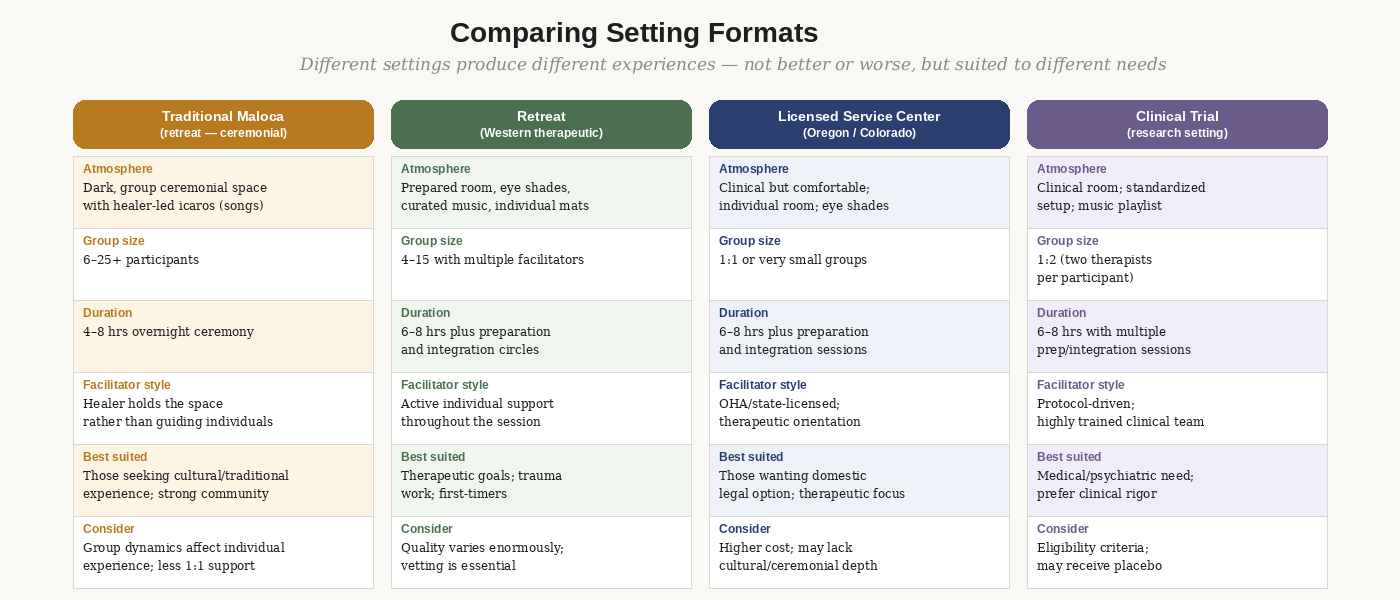
Figure 3: Major setting formats compared. No format is universally superior — the right one depends on your specific presentation, history, and goals.
The traditional maloca — ceremonial format
The ceremonial format — most common for ayahuasca and some psilocybin retreat programs — involves a group gathered in a prepared space (often a circular ceremonial hut, or maloca) with the healer or curandero leading through icaros, healing songs, and the energetic management of the space. The healer is focused on holding the collective space rather than supporting individuals moment to moment. Facilitation staff move through the group, but the primary container is held collectively.
This format has significant strengths: the shared experience creates a collective field that many participants describe as amplifying and containing; the traditional structure provides clear anchors; the group process normalizes difficulty. The limitation is individual support — with fifteen people in a maloca and three facilitators, you may have periods when support is occupied elsewhere. People who need intensive individual support during the experience may find this format more challenging.
Western therapeutic retreat format
This is the most common format for psilocybin retreat programs in Jamaica, the Netherlands, and similar destinations. Participants lie on individual mats in a prepared room, wearing eye shades, with curated music. Multiple facilitators — often one per three to five participants — move through the space providing individual support as needed. Integration circles before and after are standard.
This format tends to produce more individual therapeutic work because the structure supports internal focus rather than collective ceremony. The music is typically curated to follow an intentional arc — building in intensity toward a peak and gradually descending — which supports the experience's trajectory. The eye shades and horizontal position create an internal rather than external orientation. This is the format most closely aligned with clinical research protocols.
Licensed service centers — Oregon and Colorado
As of 2024, Oregon has fully operational licensed psilocybin service centers and Colorado is opening its first centers under Prop 122. These are regulated by state health authorities, require licensed facilitators with standardized training, and offer the only fully domestic legal psilocybin option outside clinical trials.
The format is typically individual or very small group. The facilitator is with you throughout the session. The setting is often carefully designed — comfortable, with attention to light, sound, and natural elements — but is clinical in the sense that the program is standardized and regulated. For people who want domestic access, strong facilitator regulation, and a therapeutic orientation without traveling internationally, this is the most accessible option.
Group vs individual sessions
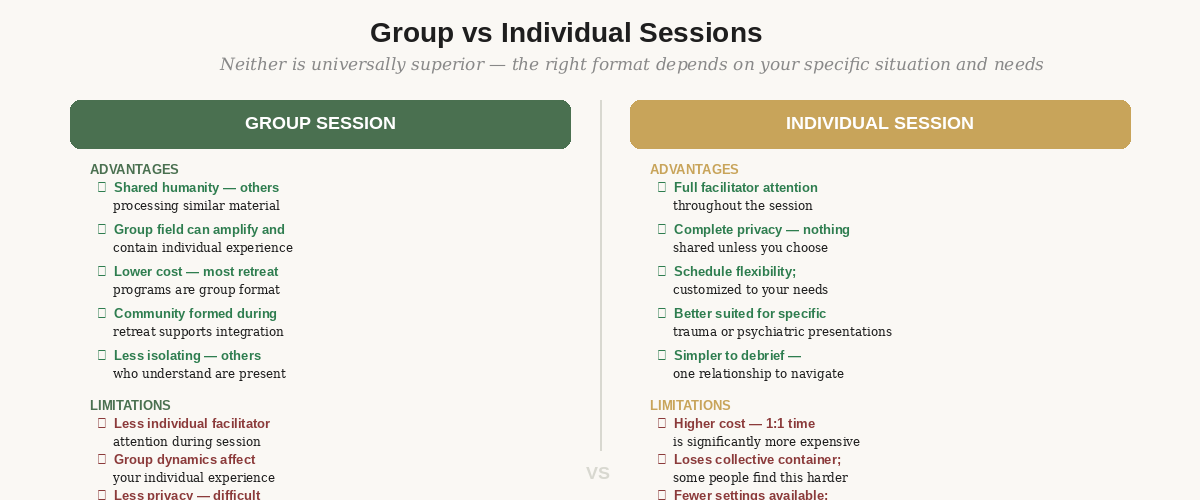
Figure 4: How the group dynamic changes the session experience — what it adds, what it requires, and when individual format is more appropriate.
The group versus individual question is one of the most practically important decisions people make and one of the least systematically thought through. Most retreat programs are group format because group format is economically viable at reasonable price points. Individual sessions are significantly more expensive because you are paying for exclusive facilitator time.
For most people with moderate preparation and no significant contraindications, group format works well. For people with significant trauma histories — particularly sexual trauma, where privacy in difficult moments is more important — or for people whose material is particularly private or complex, individual sessions deserve serious consideration. The additional cost is real; so is the additional individual support.
What You Can Control in Your Setting
Even if you've already booked a program and its format is fixed, there are aspects of setting that remain within your control. These are worth attending to specifically.
Your physical comfort items
Most programs allow and encourage participants to bring comfort items. These are not trivial — physical comfort objects create a sensory anchor to safety during the experience. Consider:
- An eye mask or shade — even if the program provides one, your own feels more personal and comfortable.
- A comfort object from home — something small that carries positive association. A stone, a piece of jewelry, a photograph.
- A thin blanket or shawl — temperature regulation becomes important when you're lying still for hours.
- Your intention card — a small piece of paper or card with your working intention written on it.
- Comfortable, loose clothing in natural fibers. Synthetic materials become uncomfortable over hours.
- Nothing that requires managing — no wallet, no keys, no devices. Simplify what you bring.
The music question
Many retreat programs use curated music as part of the facilitation structure. The music is not background — it is an active element of the container. Research from Johns Hopkins has shown that music is one of the most powerful set-and-setting variables, and their curated playlists have been specifically designed to support particular phases of the experience.
If you have any influence over the music — in an individual session or a flexible program — consider what emotional and sonic environment supports your specific work. Tracks with lyrics in your native language tend to capture attention cognitively; primarily instrumental or unfamiliar-language music allows the experience to proceed without verbal anchors. Tracks with extreme dissonance or aggression can amplify difficult material in ways that may be productive or overwhelming.
In most retreat programs, the music is curated by the facilitator and not within your control. What is within your control: listening to the program's playlist before your retreat if they share it, so the music feels familiar rather than alien when the experience begins.
Your relationship with the other participants
In a group format, the other participants are part of your setting. You will share a space with people who are also working with intense emotional material. This is usually not a problem — most people in retreat settings are navigating their own internal landscape with limited awareness of others. Occasionally, one participant's process will be audible or disruptive.
Preparation for this: know that it can happen and decide in advance how you'll respond. An internal phrase like "they're doing their work; I'm doing mine" can help redirect attention when you notice yourself pulled out of your own experience by what someone else is going through. If another participant's process becomes significantly disruptive, signal your facilitator — managing group dynamics is their job.
Communicating With Your Facilitator Before the Session
The pre-session conversation with your facilitator is one of the most underinvested preparation elements. Most people treat it as a logistics call — find out what to bring, confirm the schedule, ask basic questions. It can and should be significantly more than that.
Your facilitator needs to know specific things about you before your session, not during it. The session itself is not the time to establish this context — you will be in an altered state and your facilitator will be focused on support, not information-gathering. The intake call is the moment to ensure that the person responsible for your safety has the information they need to support you well.
What your facilitator needs to know before your session:
Your working intention — not the polished version, but what you're actually hoping to work with.
Any psychiatric history, including medications, hospitalizations, and diagnoses.
Any trauma history that is likely to be relevant — not a complete history, but the material that is most active for you right now.
Any tendency toward dissociation, and what it looks like when it happens.
What helps when you're activated — and what doesn't.
Any physical conditions that might affect the session (chronic pain, hearing sensitivity, movement limitations).
Who knows you're there and how to reach them in an emergency.
Any concerns about the session that you haven't been able to resolve.
The thing most people avoid in this module is raising genuine concerns with their facilitator.
There is a version of the pre-retreat call that is a performance of readiness — giving the "right" answers, not mentioning the thing that's actually worrying you, downplaying psychiatric history to avoid being turned away. This performance is understandable and also, in some cases, dangerous.
The facilitator's job is your safety. They cannot do that job without accurate information. The things you're most tempted to minimize — a psychiatric history that feels embarrassing, a medication you haven't fully tapered, a dissociation pattern you're hoping won't come up — are often the things that matter most for the facilitator to know.
If you're afraid that honest disclosure will get you turned away: a program that turns you away based on information that constitutes a genuine contraindication is protecting you, not rejecting you. A program that accepts you without adequate screening and something goes wrong is a far worse outcome.
Exercise: Pre-Session Facilitator Conversation Guide
Time required: 30 minutes to complete the written preparation; 15–20 minutes for the actual call.
When to do this: Complete the written portions 48 hours before your pre-retreat call with your facilitator.
Purpose: Ensure your facilitator has the information they need — and that you communicate it clearly rather than forgetting it in the moment.
The pre-session call is not a test. It is the beginning of the therapeutic relationship. Approach it as a conversation, not a performance. The goal is mutual understanding — they need to understand what you're carrying, and you need to understand what support they can provide.
Part A — Prepare what you want to communicate
Write brief answers to each of the following before the call. Don't read them verbatim — use them to make sure you cover what matters.
- My working intention in one or two sentences:
- The most important thing my facilitator should know about my mental health history:
- Current medications and what my physician has said about them:
- Patterns I have that might show up during the session (dissociation, shutdown, intense emotional expression, fear of losing control):
- What has helped me when I've been emotionally activated in the past:
- What has not helped or has made things worse:
- My biggest concern or fear about this session — the thing I haven't been able to fully resolve:
- What I'm hoping to experience or understand:
Part B — Questions to ask your facilitator
Use these to evaluate whether the program and facilitator can provide what you need:
- What does your protocol look like if a participant becomes overwhelmed or needs significant support during the session?
- How will you know if I'm in productive difficulty versus overwhelm that requires intervention?
- Given what I've told you about my history, is there anything you want to flag or prepare for specifically?
- What integration support is available in the days immediately after — not just the morning-after circle?
- Is there anything about what I've shared that makes you recommend a different approach, medicine, or timing?
Part C — After the call
Write a brief note after the call:
- What did you learn about the facilitator's approach that you didn't know before?
- Did anything they said shift your sense of readiness or concern?
- Is there anything you held back that you wish you'd said? If so — can you reach out to add it before the retreat?
- On a scale of 1–10, how much do you trust this facilitator to support you well during a difficult moment?
If your trust score is below 6 — that's worth sitting with. It may mean you need more information. It may mean the relationship needs more time. It may mean this is not the right facilitator for you. Your intuition about this is relevant data, not noise.
The 24 Hours Before Your Session
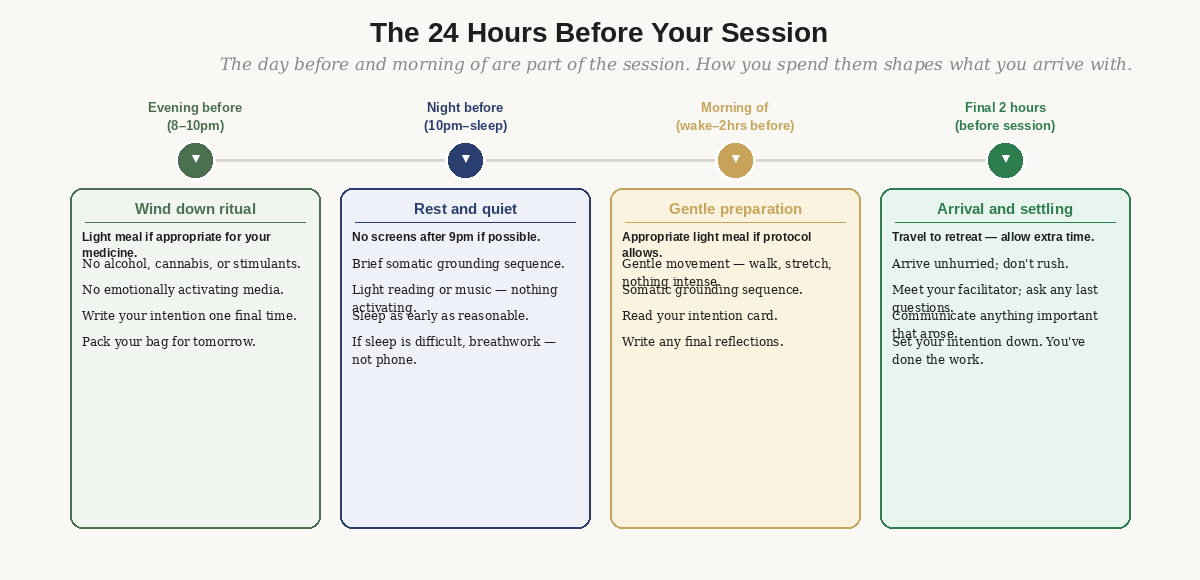
Figure 5: The final 24 hours — physical, emotional, and practical protocol.
The most important things for the evening before:
- No alcohol, cannabis, or stimulants. The night before is not the time for "one drink to calm your nerves" — alcohol disrupts REM sleep and creates a compromised nervous system baseline.
- No emotionally activating media — news, conflict-heavy films, anything that leaves you agitated or disturbed before sleep.
- Write your intention one final time. Read it. Set it down.
- Pack what you need. Arriving with logistical stress adds an unnecessary burden on the day.
- Sleep as early as is natural for you. Eight hours of rest makes a significant difference.
The most important things for the morning of:
- The appropriate meal for your medicine — see Module 3. Not too much, not nothing.
- Gentle movement only. A walk, some stretching. No intense exercise.
- The somatic grounding sequence from Module 4.
- Read your intention card one more time — then consciously set it aside.
- Arrive with time to spare. Arriving rushed adds activation the experience will amplify.
What to do in the final two hours:
- Meet your facilitator unhurried. Ask any last questions.
- Communicate anything that has come up in the past 48 hours that is relevant — recent dreams, concerns, emotional material that has surfaced.
- Tell your facilitator specifically how to help you if you're in difficulty — a hand on the shoulder, a verbal check-in, a specific phrase.
- Set your intention down. You have done the preparation. The session will work with what you've built.
- Have you completed a pre-retreat call or conversation with your specific facilitator — not just an intake coordinator?
- Have you answered the facilitator conversation guide questions honestly, including the things you were tempted to minimize?
- Do you know specifically what the facilitator will do if you become overwhelmed during the session?
- Do you have your comfort items identified and ready?
- Is your 24-hour plan written out — specifically what you will do the evening before and morning of?
Resources
Research
Carhart-Harris, R. et al. (2018). Psilocybin with psychological support for treatment-resistant depression: six-month follow-up. Psychopharmacology, 235(2), 399–408. Demonstrates the role of mystical experience quality — directly shaped by set and setting — in treatment outcomes.
Hartogsohn, I. (2017). Constructing drug effects: A history of set and setting. Drug Science, Policy and Law. The most thorough historical and scientific review of the set and setting concept.
Practical
Johns Hopkins Psychedelic Research Unit (hopkinspsychedelic.org) — music playlists and preparation materials from the research protocols. Publicly available.
MAPS MDMA Therapy Training Manual (available at maps.org) — the preparation and facilitation protocols from Phase 3 clinical trials. Provides the clearest picture of what rigorous therapeutic facilitation looks like.
For evaluating programs
Retreat Guru and Psychedelics.com maintain user reviews and vetting information on international retreat programs. HealingMaps (healingmaps.com) specializes in North American programs. Cross-reference multiple sources rather than relying on a single directory.