Inside the Session — Navigating the Experience
- Understand why intellectual preparation cannot fully prepare you for a psychedelic session — and what kind of preparation actually can.
- Know the experience arc across all five major medicines, including what to expect at onset, peak, descent, and return.
- Have a clear, practiced framework for working with difficulty during the session — including the specific distinction between productive difficulty and overwhelm.
- Know how and when to signal your facilitator, and why doing so is a sign of preparation rather than failure.
- Have completed the session intention card and anchor practice — two small but significant tools for the session itself.
Opening
This module is the pivot point of the course. Everything before it was preparation. Everything after it is integration. This module lives in the threshold between those two phases — which means it has to do something unusual: prepare you for an experience that genuinely cannot be fully prepared for.
That sounds paradoxical. It isn't. There is a difference between intellectual preparation — understanding what ayahuasca does to serotonin receptors, knowing that purging is normal, reading accounts of what other people experienced — and experiential preparation. Intellectual preparation is necessary and insufficient. It gives you a map. The experience is not the map. When the intensity arrives, the intellectual knowledge tends to recede, and what remains is your actual capacity — your window of tolerance, your relationship with breath, your ability to be present with difficult material without fighting it. That capacity is what Modules 3 through 5 have been building.
What this module adds is specific: the tools and orientations for use during the session itself. Not intellectual frameworks to think through mid-experience — thinking is exactly what gets disrupted. Instead: simple physical anchors, a practiced decision sequence for navigating difficulty, clarity about when to stay with something and when to signal for help, and understanding of how the session arc typically unfolds so you're not surprised by the structure of what you're moving through.
One note before we begin: this module is written for a general audience across multiple medicines. The experience of psilocybin in a therapeutic retreat is significantly different from MDMA in a clinical setting, which is different from a multi-day ibogaine treatment. Where important differences exist, they're noted. But the core navigation principles — surrender, breath, presence, the productive-difficulty distinction, working with the facilitator — apply across all formats.
What You Cannot Prepare for Intellectually — and What You Can
The most honest thing that can be said about this module is also the most counterintuitive: reading it will not fully prepare you for the experience. No amount of reading will. The experience operates in registers of perception and emotion that are genuinely different from ordinary waking consciousness, and intellectual familiarity with those registers is not the same as being in them.
What reading this module can do:
- Give you a framework for what is happening when it is happening — so the experience doesn't feel random or meaningless even when it is disorienting.
- Build familiarity with the tools you'll use — breath, grounding, the session anchor — so they are practiced and available, not newly encountered.
- Reduce surprise, which is one of the primary contributors to difficulty. Surprise and intensity are different things. An experience can be intensely difficult without being surprising, and that distinction matters enormously in how you navigate it.
- Give you permission, explicitly, to signal your facilitator when you need support — which many people don't feel they have and therefore don't use.
What experiential preparation can do — and what the practice in Modules 3 through 5 has been building:
- A wider window of tolerance — more capacity to be present with intensity without flooding.
- A practiced relationship with breath — accessible as an anchor even when cognitive resources are occupied.
- Some familiarity with your own internal landscape through the dark room practice and journaling.
- An intention that creates gravity — a direction the medicine can pull toward, and something to return to if you lose your bearings.
The Experience Arc
Understanding how the experience typically unfolds across time — the arc from onset through peak to return — reduces one of the most common contributors to difficulty during sessions: not knowing where you are in the arc, and therefore not knowing whether what's happening is the beginning, the worst of it, or the beginning of the end.
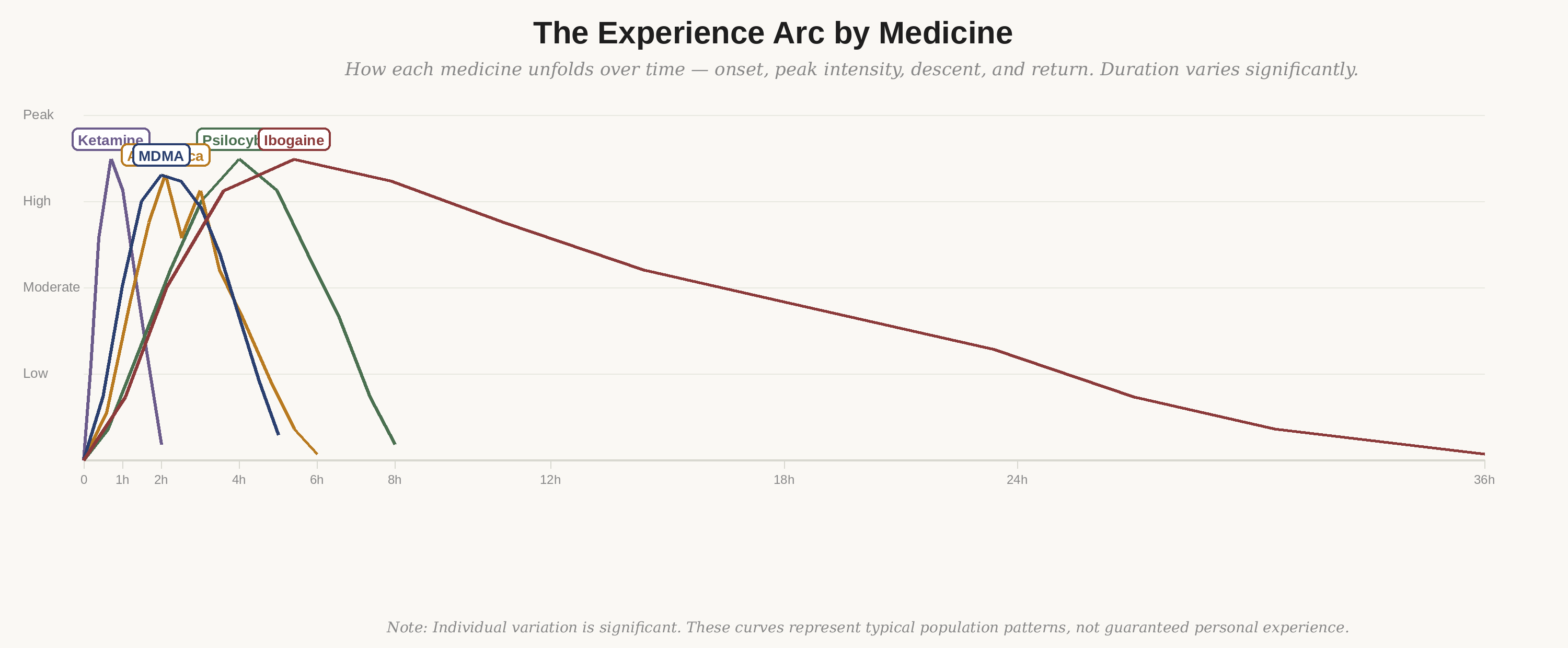
Figure 1: How each medicine unfolds over time — onset, peak intensity, descent, and return. Individual variation is significant.
Onset — the medicine arriving
Onset — the period between ingesting the medicine and the beginning of significant effects — is often when anxiety peaks. You have crossed the threshold, you cannot uncross it, and you don't yet know what's coming. The body may feel heavy or warm. There may be nausea, particularly with ayahuasca. Subtle visual changes may appear at the edges — colors slightly brighter, geometric patterns beginning to form behind closed eyes.
The most useful orientation at onset: be patient. The medicine is arriving on its own timeline. Anxiety about when it will arrive, whether it's working, whether you took enough — all of this is the ordinary analytical mind trying to maintain its usual orientation. This is exactly what will be interrupted. The arrival is happening. Focus on breath. Keep eyes closed or softly unfocused. Let it come.
One medicine-specific note: ketamine arrives much faster than the others — the full effect of an IV infusion is typically felt within five minutes of the infusion beginning. MDMA has a longer onset of 45–90 minutes before full effects are felt. Psilocybin typically takes 20–60 minutes. Ayahuasca varies considerably based on the brew and individual metabolism.
Peak — the work
The peak is the period of highest intensity. It varies by medicine in character, duration, and content. For psilocybin, the peak is typically one to three hours into the session and lasts one to two hours. For MDMA, the peak is longer and characterized less by visual intensity than by emotional opening. For ayahuasca, there may be multiple waves of intensity across the ceremony — the peak of one wave subsides, and another arises.
At peak intensity, ordinary cognitive processing is significantly reduced. This is the point. The default mode network — the self-referential, analytical mind — is quieted, creating a window in which other material can surface. What surfaces is not random — it's shaped by your intention, your history, and the specific material your system has been holding. It will often be more intense than you expected, more emotionally raw, less orderly, and more genuinely significant than anything you prepared for intellectually.
The primary orientation at peak: you do not need to understand what's happening while it's happening. You need to be present with it. The understanding comes later, during integration. At peak, the task is to receive rather than analyze — to let what wants to arise arise, without grabbing it to examine it or pushing it away because it's uncomfortable. This is the moment when everything in this course converges: the widened window of tolerance, the practiced breath, the surrender orientation.
Descent — the return begins
The descent from peak intensity is gradual and nonlinear — it is common to have a period of relative clarity followed by another wave, particularly with ayahuasca. The descent is characterized by a gradual return of ordinary cognitive functioning. Colors return to normal. The sense of being located in a body and a space becomes more stable. Insights that were vivid during the peak begin to crystallize into language.
The most common mistake during descent: rushing toward ordinary consciousness. There is often a significant relief in the intensity reducing, and that relief creates a pull toward returning to normality — reaching for the phone, wanting to talk, wanting to be "back." Resist this pull. The descent is part of the work. What crystallizes in the descent is often among the most integrable material from the session. Stay with it.
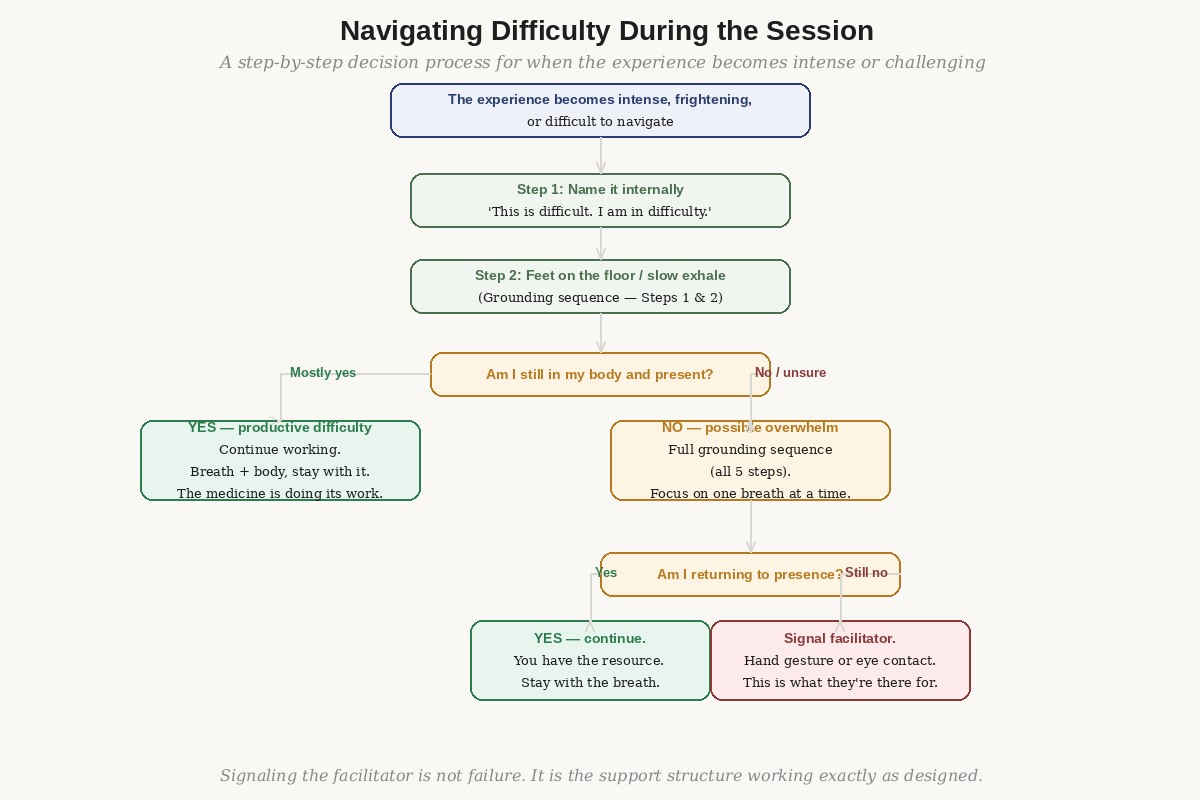
Figure 2: A step-by-step decision process from naming the difficulty through the full grounding sequence to signaling the facilitator.
The return — first hours after
The hours immediately after a session are a specific state — not ordinary consciousness, not the session, but something in between. The acute effects have subsided, but the elevated neuroplasticity persists. This period has a particular quality of openness and sensitivity that is worth protecting.
In most retreat programs, the morning after ceremony includes an integration circle — a facilitated group sharing of what arose. This is not optional, and its value is not fully apparent until you're in it. Hearing others describe their experiences contextualizes and normalizes your own. Something you experienced in isolation becomes part of a shared human field. This is part of why the group format retains therapeutic value even for people whose primary work is individual.
In the first hours after the session: eat something small if you feel any capacity for it. Not a full meal — something light and nourishing. Drink water. Move gently. Spend time in nature if it's available. Write a few notes — not a full journaling session, but the images, phrases, or insights that feel most charged. These notes are for you to return to in the days following; they will mean more then than the effort of writing them feels worth now.
The Surrender Principle in Practice
The surrender principle — the orientation of allowing what arises to arise rather than fighting it — has been introduced in Module 4. Here we look at what it actually means to practice it during a session, when intellectual understanding is reduced and the practice must be embodied rather than conceptual.
Surrender is not passive collapse. It is an active choice, made repeatedly, to meet what is arising rather than fighting it. The experience doesn't stop when you fight it — it intensifies, because resistance is itself arousal, and arousal amplifies the very content being resisted. Surrender is the discovery that difficult material, when not fought, tends to move through rather than remain. It is the experiential confirmation of the weather metaphor from Module 4: you are not the weather. The weather passes through you.
What surrender looks like physically
Practically, surrender during a session looks like this: you notice the body tensing against something. Jaw clenching, shoulders drawing up, hands making fists, breath shortening. You recognize this as resistance. You deliberately soften — jaw, shoulders, hands, and most importantly, the exhale. You lengthen the exhale. You let the body return toward horizontal. You stop trying to understand what is happening and return to simply feeling it.
This is easier said than done at high intensity. It requires having practiced the body scan and breath sequence enough that the instruction "soften and exhale" activates a familiar physiological response rather than a new cognitive task. This is the reason Module 4's daily practice is not optional.
Surrender and the specific content that arises
Surrender doesn't mean passivity about what the medicine surfaces. When grief comes, it doesn't mean suppressing it — it means letting it move. When anger arises, it doesn't mean expressing it physically — it means letting it be felt without acting on it or shutting it down. When fear arrives, it doesn't mean pretending not to be afraid — it means feeling afraid and not fighting the fear.
The functional version of surrender in each case is: "I feel this, and I am still here, and it is allowed to be here." That sentence, held internally, is more useful during a difficult moment in a session than any intellectual framework. It's worth memorizing it as a phrase before you go.
Breath as the Primary Tool
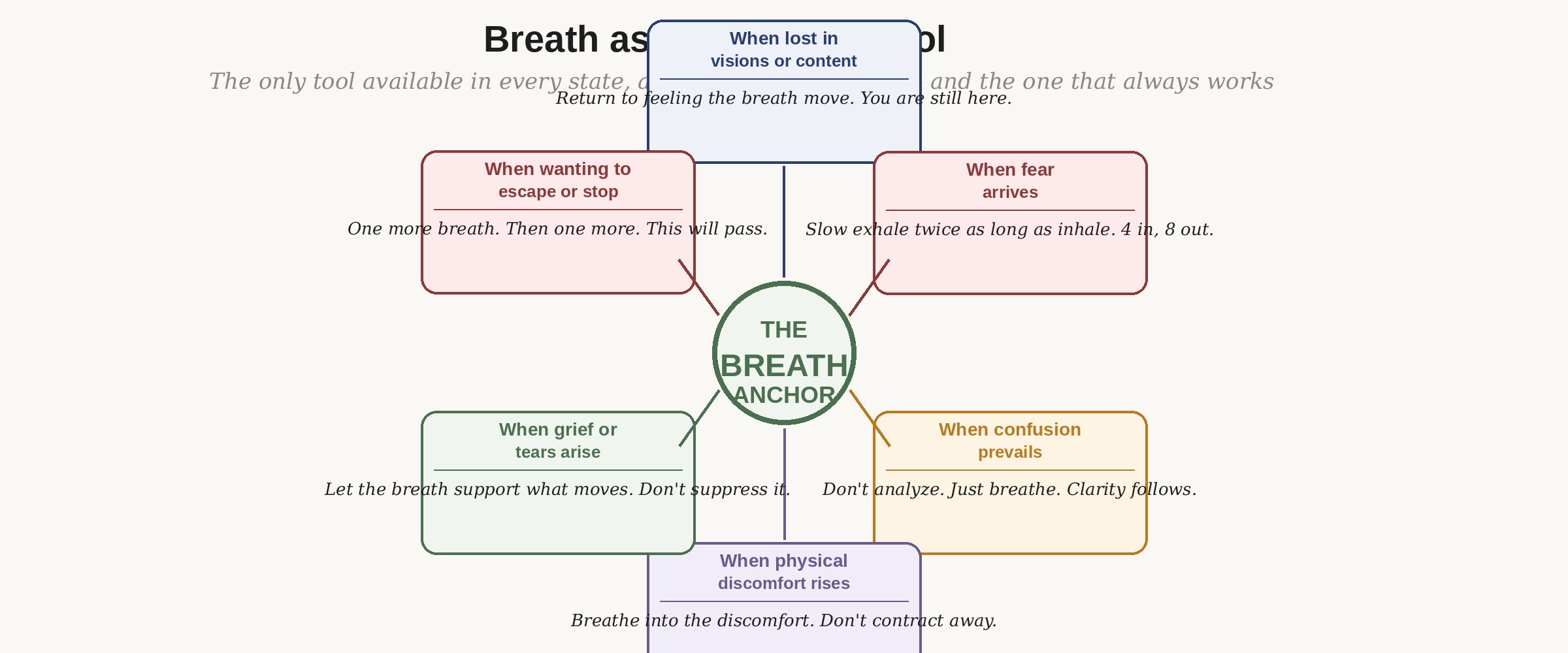
Figure 3: The breath anchor — available at every intensity level, requiring the least cognitive capacity of any tool.
The breath is the only tool that is available in every state — at every intensity level, whether you are in productive difficulty or approaching overwhelm, whether you have full cognitive access or very little. It is also the tool that takes the least cognitive capacity to use. In a state where abstract reasoning is significantly reduced, "feel the exhale" is a simpler instruction than almost anything else that could be offered.
There is also a physiological reason the breath is primary. As Module 4 explained, the extended exhale directly activates the parasympathetic nervous system — the branch responsible for rest and recovery, as opposed to the sympathetic fight-or-flight branch. Every time you extend the exhale during a session, you are directly intervening in the arousal cascade that, unchecked, leads from intensity to overwhelm. This works physiologically even when it doesn't feel like it's working subjectively.
The primary breath instruction for sessions
If you remember nothing else from this module: when in doubt, exhale longer than you inhaled. Four counts in; eight counts out. Or whatever ratio feels possible — the point is the exhale being longer than the inhale. Do this three times before doing anything else. This is the first step of the difficulty navigation sequence, and it is sufficient for many difficult moments without requiring anything further.
Distinguishing Productive Difficulty from Overwhelm
This distinction is the most practically important skill in this module. It determines whether you continue working with what's arising or signal for support. Getting it wrong in either direction is costly: mistaking productive difficulty for overwhelm leads to ending a productive process prematurely; mistaking overwhelm for productive difficulty means staying alone with something that requires support.
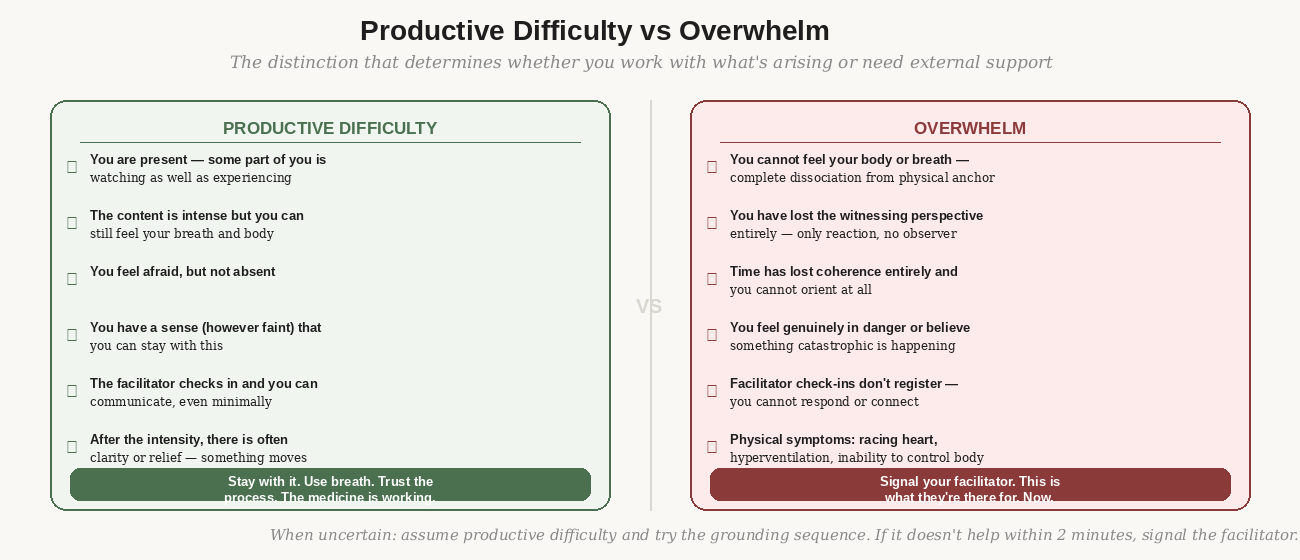
Figure 4: The six markers that distinguish productive difficulty (stay with it) from overwhelm (signal the facilitator).
The witnessing perspective — the key marker
The single most reliable indicator of the distinction is the presence or absence of the witnessing perspective: the part of you that is observing the experience as well as having it. In productive difficulty, this witness is present, however faint. You may be in terror — but some part of you knows you're in terror, which means there is an observer present. You may be in profound grief — but some part of you is watching yourself grieve.
When the witnessing perspective disappears entirely — when you are only the experience with no observer, no sense of being a person having an experience — this is closer to overwhelm. The medicine has gone further than your current window of tolerance supports. This is not a failure or a crisis — it is information, and it is the moment to use the grounding sequence and, if that doesn't return the witness within a few minutes, to signal your facilitator.
The practical decision sequence
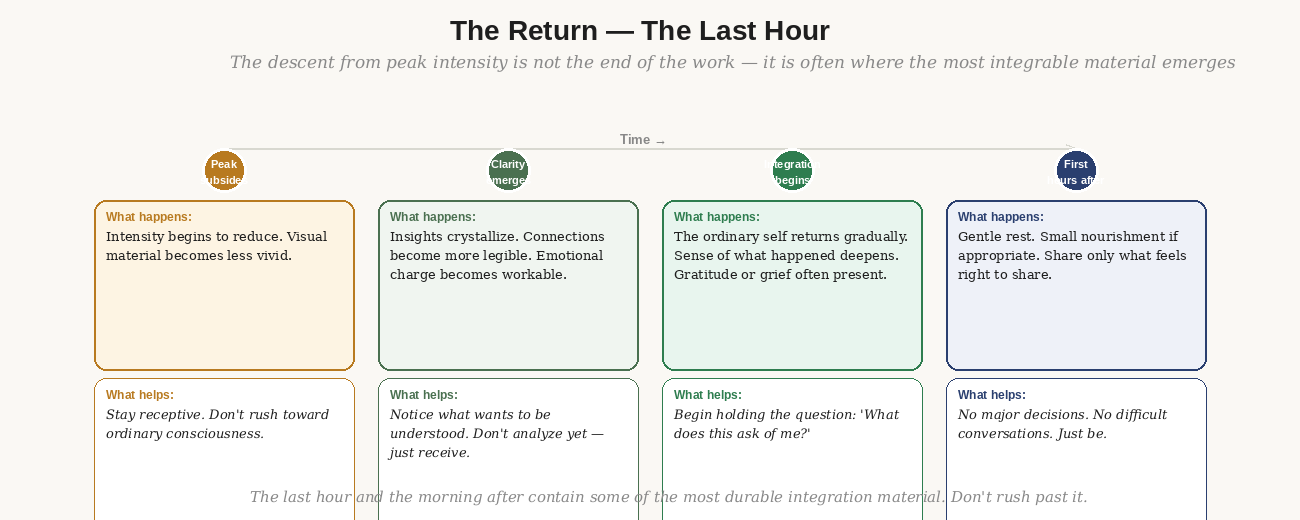
Figure 5: The descent and return — not a recovery period but often where the most durable integration material crystallizes.
When the experience becomes significantly difficult:
- Name it internally: "This is difficult. I am in difficulty." This is not catastrophizing — it is the first act of witnessing. You are naming the state rather than being entirely consumed by it.
- Feet on the floor / slow exhale. The first two steps of the grounding sequence. Don't think about them — just do them. This takes thirty seconds.
- Check: can I feel my breath and body? Am I still in some sense present? If yes, continue with what's arising. If no — or deeply uncertain — do the full five-step grounding sequence.
- After the full sequence: am I more present? If yes, continue. If no — signal the facilitator. A hand gesture, eye contact, or the pre-agreed signal you established in your pre-session conversation.
The instruction to signal the facilitator deserves its own emphasis. Many people resist signaling because they feel they should be able to handle it, because they don't want to disrupt others, because they're in a state where communication feels impossibly difficult. The facilitator is watching. They want to know. Signaling is not failure — it is using the support structure you have spent significant preparation effort building. A good facilitator will read even subtle signals and come to you.
What's Normal, What's Uncommon, and What Needs Attention
Normal and expected
- Nausea and purging — particularly with ayahuasca, and sometimes with psilocybin. The bucket is there for a reason.
- Crying, sometimes intensely. This is emotional material moving, which is the therapeutic mechanism.
- Laughter, sometimes inappropriate-seeming. Emotional release can express through multiple channels.
- Visual phenomena — patterns, colors, imagery, formed or abstract. These are not hallucinations in the clinical sense; they are perceptual effects of 5-HT2A activation.
- Feeling significantly larger or smaller than your body. Distortion of body image is common.
- A sense of time distorting dramatically — an hour feeling like minutes or decades.
- The sense that something deeply significant is happening, even when the content seems ordinary.
Less common but not concerning
- Intense physical sensation — warmth, electricity, vibration in the body.
- Apparent encounters with entities, presences, or other beings. Reported commonly, understood poorly. You don't need to resolve what these are; you need to be able to be with them.
- Ego dissolution — the sense of the ordinary self dissolving or disappearing. This is often frightening and often among the most therapeutically significant experiences.
- Profound visual complexity — geometric patterns of great detail, sometimes landscape-scale imagery.
- A sense of life review — autobiographical memories arising in sequence.
Requires facilitator attention
- Inability to be present or communicate at all after the full grounding sequence — complete dissociation.
- Physical symptoms beyond nausea: chest pain, difficulty breathing that doesn't respond to breath work, significant involuntary movement that is distressing.
- Persistent belief that something catastrophic is happening in external reality — not internal imagery but a fixed belief about the actual world.
- Loss of any sense of the experience being temporary.
A note on entity encounters and ego dissolution:
These are the two experiences people are most unprepared for and most afraid of. Neither is inherently dangerous. Both are well-documented in psychedelic research and in contemplative traditions that have worked with non-ordinary states for millennia.
Ego dissolution — the temporary loss of the sense of being a separate self — is consistently the experience most strongly correlated with positive therapeutic outcomes in psilocybin research. It is also the experience most likely to feel terrifying before it happens and most likely to feel profound after it does.
Entity encounters are reported by a significant proportion of people working with psilocybin and ayahuasca. The research has nothing definitive to say about what they are. What is clear is that resisting them tends to prolong and intensify them; engaging with them curiously tends to allow them to move. The same surrender principle that applies to emotions applies here.
Communication With Your Facilitator During the Session
Before your session, you will have established how to signal for support. Most programs use eye contact, a hand gesture, or a simple verbal signal. Whatever was agreed — remember it, and use it without hesitation when you need it.
During the session, your facilitator may check in with you periodically. Common check-in approaches include a gentle hand on the shoulder, quiet eye contact, or a brief verbal "are you okay?" They are not expecting a coherent verbal report. A nod, a hand gesture, a single word — "difficult" or "okay" — is sufficient communication. The facilitator reads a great deal from your physical state that doesn't require words.
If you need more active support — you want them nearby, you want to talk briefly, you want physical grounding — communicate this as directly as you can in the state you're in. Pointing toward them, reaching out a hand, making sustained eye contact. Skilled facilitators are trained to read these signals and respond appropriately.
What you should not do: white-knuckle through severe overwhelm for hours because you don't want to "bother" your facilitator. The facilitator is not an obstacle to a pure solo experience. They are part of the therapeutic container. Using them is not failure — it is using the session correctly.
The thing people most want to avoid in this module is genuinely sitting with the possibility that the experience will not be what they expect.
There is a version of preparation that is elaborate psychological management — trying to ensure, through thorough preparation, that the session will go a particular way. It will not. The medicine is not obligated to deliver what you prepared for. It will find what is there, which may include material you didn't know was there, material you were hoping had been dealt with already, or material that arrives in a form that bears no resemblance to what you anticipated.
The hardest thing this module asks: can you prepare thoroughly and then let go of the preparation? Can you do the work of setting your intention, building your capacity, choosing your setting carefully — and then, at the threshold, release the grip? The preparation creates the conditions. It does not control the outcome.
Whatever arises is the material. Whatever arises is workable. You have been preparing to meet it.
The Session Intention Card
Time required: 15 minutes.
When to do this: The evening before your session.
Materials: A small card or piece of paper — something that fits in your hand.
This exercise takes the working intention you've been developing since Module 2 and distills it to its essence — a single sentence, or at most two, that captures the direction you're pointing without the complexity of the full intention work.
The purpose of the card: it is not a script to read during the session. It is a last point of contact with your preparation before you enter the session. Most people read it during the final quiet moments before the medicine is served, then set it aside — physically and psychologically. You have done the priming work. The card reminds you of that before you release it.
How to write the card
- Take out your full working intention from Module 2. Read it.
- Ask: what is the single most essential part of this? The one phrase or question that is most honest and most important.
- Write that — and only that — on the card. Keep it to one sentence. If possible, phrase it as a question or an open direction rather than a statement. Examples:
- Keep the card with you — in your pocket or in your hand — during the session preparation. Read it when the medicine is about to be served. Then fold it and set it aside, physically. You've done the priming. Now let the session begin.
The Anchor Practice
Time required: 10 minutes to identify; practiced daily in the week before your retreat.
Purpose: A single word or brief phrase that functions as a return point during the session when you lose your bearings.
The anchor is different from the intention. The intention is directional — it points toward what you're working with. The anchor is stabilizing — it returns you to present-moment ground when you've been carried away by the current of the experience.
The anchor is a single word or very short phrase that, when you say it internally, activates a felt sense of stability. It works through association: you build the association between the word and a state of groundedness in the week before your retreat, so that during the session, when you say the word, the body recognizes it.
How to choose your anchor
Your anchor should be:
- A single word or at most four words — short enough to remember and use without cognitive effort.
- Associated with something that reliably activates a felt sense of safety or stability for you.
- Not a command ("calm down") — but a return ("here," "ground," "breath," your name).
- Personally meaningful — words that carry weight for you specifically, not generic "peace" or "love."
Common effective anchors: a person's name (someone who represents safety for you), a place (a specific natural setting that you associate with stability), a single quality ("here," "present," "ground"), or a brief phrase ("I am still here," "this will pass," "one breath").
Building the association before your retreat
For the seven days before your retreat, at the end of each somatic grounding sequence (from Module 4):
- Arrive at the end of Step 5 — hand on chest and belly, settled breath.
- Say your anchor word internally, three times, slowly.
- Feel whatever arises in the body when you say it. Notice the quality of settledness, if it's there.
- Repeat the anchor again once. Then complete the practice.
This builds a conditioned association between the word and the physical state of groundedness. During the session, when you say the anchor internally, the body has seven days of practice connecting that word to this state. It will not work perfectly — nothing does at peak intensity — but it will work enough.
Using the anchor during the session
When you feel yourself being carried away from any sense of ground — when breath is insufficient alone, when the witnessing perspective is very faint — say your anchor internally. Three times, slowly. Then feel for your breath. Then feel for your feet or the back of your body on the mat. This sequence — anchor, breath, body — is the short form of the full grounding sequence, compressed for use when cognitive resources are minimal.
- Before the session itself — and before moving to Module 7 after:
- Have you written your session intention card? Is it physically somewhere you can access the evening before?
- Have you chosen and practiced your anchor word for at least three days? Has the association begun to feel established?
- Do you know specifically how you will signal your facilitator if you need support? Have you confirmed this signal in your pre-session call?
- Can you distinguish, in principle, between productive difficulty and overwhelm? Can you name the key marker — the witnessing perspective?
- Is there any aspect of what's covered in this module that you've been avoiding thinking about? Name it.
Resources
Research
Griffiths, R. et al. (2016). Psilocybin produces substantial and sustained decreases in depression and anxiety in patients with life-threatening cancer. Journal of Psychopharmacology. Includes the Mystical Experience Questionnaire data and its correlation with positive outcomes — directly relevant to understanding what the peak experience produces.
Carhart-Harris, R. et al. (2014). The entropic brain: a theory of conscious states informed by neuroimaging research with psychedelic drugs. Frontiers in Human Neuroscience. The theoretical framework explaining what happens to brain organization during psychedelic states.
First-person accounts
How to Change Your Mind — Michael Pollan. Chapter 3 includes unusually honest first-person accounts of difficulty and ego dissolution that are useful calibration for what the experience can involve.
Acid Test — Tom Shroder. Accounts of MDMA-assisted therapy for PTSD that provide the most honest published descriptions of what navigating a difficult MDMA session looks like from inside it.
Practice tools
Johns Hopkins Psilocybin Music Playlist (available on Spotify and Johns Hopkins website) — the playlist used in research trials, specifically designed to support the experience arc. Listening before your retreat builds familiarity.
Zendo Project training materials (zendoproject.org) — the peer support and harm reduction guidance, including the "difficult experience support" protocols, are among the clearest practical guides to what facilitators do when someone is in difficulty.