The Body in Integration
- Understand why integration is not primarily a cognitive process — and why accessing the body is not supplementary but central to lasting change.
- Know the neurological basis for why conventional talk therapy has limitations for trauma integration, and what somatic approaches address that talk alone doesn't.
- Have a practical toolkit of five somatic integration practices — movement, breathwork, cold exposure, TRE, and Somatic Experiencing — with clear guidance on when to use each.
- Understand the role of sleep and dreams specifically in the integration process, and have a practice for working with both.
- Have completed the body map exercise and established the daily somatic check-in.
Opening
The mind wants to understand what happened. It wants to organize the experience into a narrative — to extract meaning, to build a story that explains what the medicine showed and what to do with it. This cognitive activity is part of integration. It is not all of it, and in some ways it is the easier part.
The body has its own account of what happened. It was present for the entire session — it held the fear, it moved through the grief, it carried the activation of difficult moments and the opening of profound ones. If you left the session and went directly into cognitive processing — journaling, thinking, talking — without returning to the body, you have only integrated half the material. The half that fits into language. The half that can be articulated.
The other half lives in the nervous system. In the muscle tension that persists after the session. In the places where you've been holding for years without knowing it. In the proprioceptive patterns that encode old relational dynamics — the rounded shoulders of chronic shame, the braced core of ongoing threat response, the shallow breathing of someone who learned early that fully inhabiting their body was not safe. The medicine often makes these patterns visible — makes them felt in a new way during the session. Integration requires following that visibility into change, and that change happens in the body as much as in the mind.
This module is the most practical in the integration sequence. It covers specific body-based tools — not as wellness supplements but as primary integration mechanisms — and gives you both the understanding of why they work and the instructions for how to use them.
Why Integration Lives in the Body
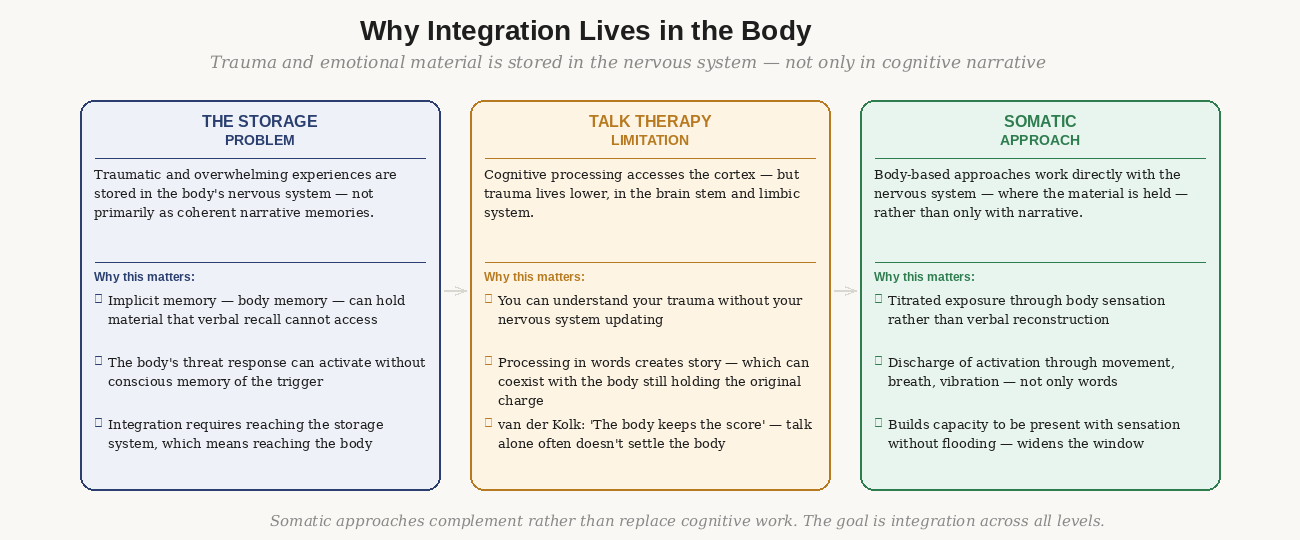
Figure 1: The neurological case — trauma is stored in the nervous system, not the cortex. Reaching it requires body-based approaches alongside cognitive processing.
The field of trauma neuroscience has produced a clear picture over the past thirty years: overwhelming experiences are encoded not primarily as narrative memories but as body states. The threat response — the physiological activation of fight, flight, or freeze — is stored in the brainstem and limbic system, not in the cortex where language and narrative live. Peter Levine, the founder of Somatic Experiencing, describes trauma as "a highly activated, incomplete biological response" — the nervous system mobilized for threat and never fully discharged.
This has a specific implication for integration: you can understand your trauma completely without your nervous system updating. You can construct an accurate narrative about why you are the way you are, identify the formative experiences, understand the patterns — and the body can continue to hold the original activation, continuing to shape behavior from outside conscious awareness. The story is complete; the nervous system hasn't received the memo.
Somatic approaches work by addressing the nervous system directly — through the body, through sensation, through movement and breath and physical contact with the present moment. They don't bypass narrative; they work alongside it, addressing the level at which the material is actually stored.
What psychedelic sessions make available
One of the reasons psychedelic integration has a somatic dimension that ordinary therapy integration doesn't is that the session itself is a body experience. The medicine produced physical effects — sensations, activation, sometimes purging or intense physical movement. The session surfaced material that was felt physically before it was understood cognitively. The body was the instrument through which the experience occurred.
This means that the body has integration material that the mind may not have access to. Physical sensations that arose during the session that were not fully processed. Areas of activation that didn't discharge during the session. The held breath, the clenched jaw, the braced core that was present during the peak — these are integration material, as much as any insight or image.
The Five Somatic Integration Practices
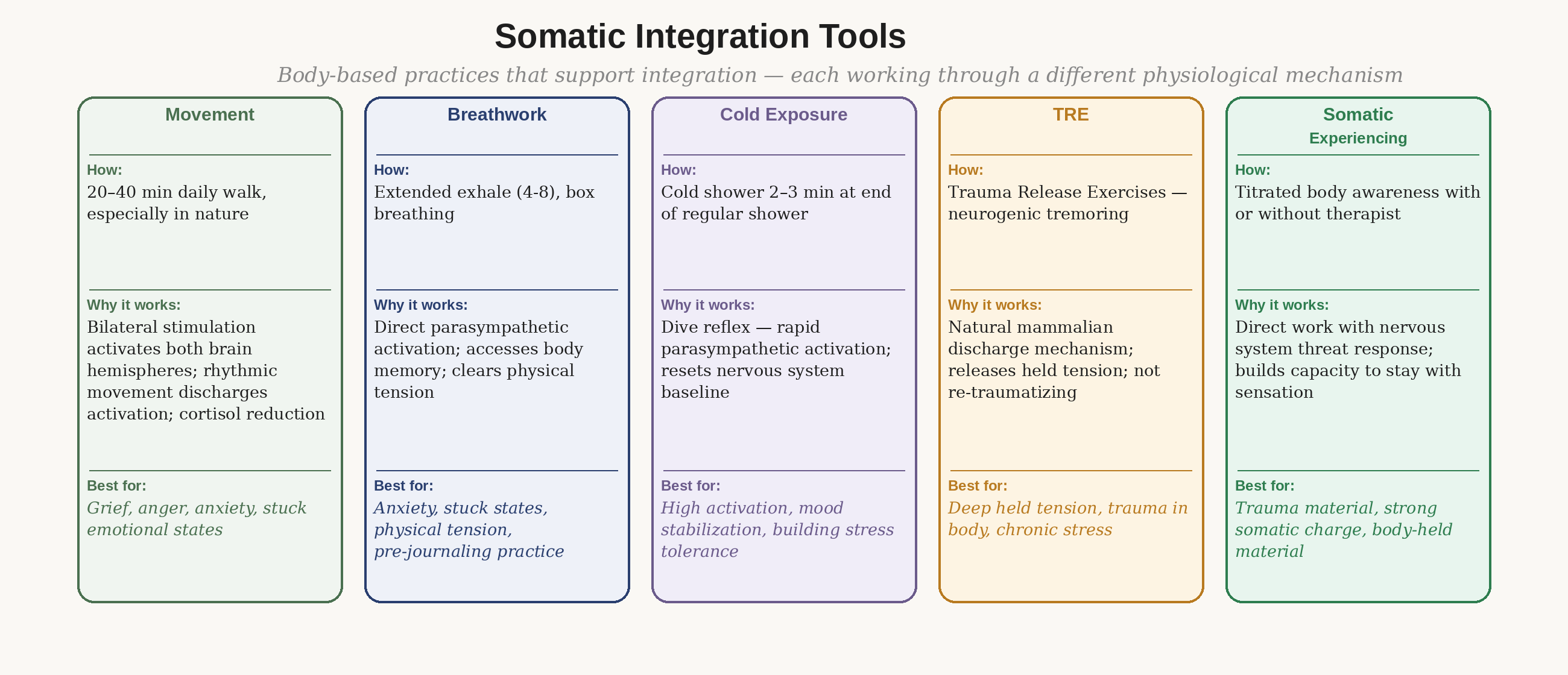
Figure 2: Five tools, five mechanisms. Each addresses a different aspect of somatic integration.
Movement and walking
Daily walking is the most accessible somatic integration practice and, for most people, the most reliable. The mechanism is bilateral stimulation — the alternating activation of left and right brain hemispheres that occurs during rhythmic bilateral movement. This is the same mechanism used in EMDR (Eye Movement Desensitization and Reprocessing), one of the most evidence-supported trauma treatments. Walking, running, swimming, and other bilateral rhythmic movement create the same bilateral processing that makes EMDR effective.
Walking in nature adds a second mechanism: cortisol reduction through the sensory environment. Research consistently shows that time in natural settings reduces cortisol (the primary stress hormone) more effectively than urban or indoor environments. During the integration window, when the nervous system is elevated and sensitive, this cortisol reduction has significant practical value.
The instruction: twenty to forty minutes of walking daily during the integration period. Preferably in nature; if not available, any outdoor movement is better than indoor. No headphones for the first fifteen minutes — allow the bilateral movement and environmental stimulation to work without competition from audio content. If processing material arises during the walk, let it arise. The movement supports the processing; you don't need to manage it.
Breathwork
The breath is the primary bridge between the voluntary and involuntary nervous systems — the only autonomic function we can also control consciously. This makes it uniquely positioned for integration: it can both respond to the nervous system's state (tight breath in anxiety) and regulate it (deliberately extended exhale reducing arousal).
For somatic integration, breathwork serves two distinct functions. The first is nervous system regulation — the extended exhale practice from Module 4, used daily to maintain the parasympathetic baseline that supports integration. The second is accessing stored material — deliberately slower, fuller breathing can surface body memories and emotional material that ordinary breathing keeps suppressed. This second function is more intense and is best approached with guidance, either from a trained breathwork facilitator or through a structured protocol.
For self-directed use during integration: the extended exhale practice (four counts in, eight out) done for ten minutes before journaling often surfaces material that the cognitive mind wouldn't have found directly. Box breathing (four in, four hold, four out, four hold) is useful for acute activation — moments when the nervous system is running high and you need to regulate quickly before engaging with the material.
Cold exposure
Cold water exposure activates the mammalian dive reflex — a hardwired physiological response that produces rapid parasympathetic activation. Heart rate slows. Vasoconstriction occurs peripherally. The nervous system, facing the physiological challenge of cold, reorganizes rapidly.
The integration application is specific: a cold shower at the end of a regular shower (two to three minutes of genuinely cold water, not just slightly cooler) produces a brief parasympathetic surge that is useful for mood stabilization, resetting a nervous system that has been running high, and generating mild alert energy without cortisol elevation. It is not a cure for destabilization or grief — it is a nervous system reset tool with a specific useful function.
Build gradually: end regular showers with thirty seconds of cold, then sixty, then two to three minutes over the first week. The discomfort is part of the mechanism — it builds tolerance for uncomfortable physical sensation, which is directly relevant to building tolerance for uncomfortable emotional sensation during integration.
TRE — Trauma and Tension Release Exercises
TRE was developed by David Berceli and is based on the observation that animals, after an encounter with threat, naturally tremble and shake as part of discharging the activation of the threat response. Humans inhibit this tremoring — we've learned to hold still, to suppress visible signs of activation. This suppression may interrupt the natural completion of the nervous system's threat response.
TRE uses a series of simple exercises that fatigue specific muscle groups in a controlled way, triggering the body's natural neurogenic tremoring response. The tremoring is involuntary once initiated — the body does it, you don't perform it. It is not re-traumatizing and doesn't require talking about or cognitively engaging with the material being released. It is the body discharging activation that has been stored physically.
TRE is best learned initially with a certified TRE provider, who can guide the first several sessions and help you regulate the tremoring if it becomes too intense. After that, it can be practiced independently. For people who carry significant physical tension or trauma held in the body, TRE can produce experiences of release that feel simultaneously physical and emotional — crying, shaking, warmth, and a subsequent sense of calm.
Somatic Experiencing
Somatic Experiencing (SE), developed by Peter Levine, is a body-based approach to trauma that works by titrating exposure to somatic charge — building the person's capacity to be present with body sensation associated with traumatic material without flooding. The core concept is pendulation: moving attention between areas of activation (where the charge is held) and areas of resource (where the body feels safe and stable), gradually building the capacity to stay present with increasing levels of activation without the nervous system going into overwhelm.
SE is most effectively practiced with a trained SE practitioner, particularly for significant trauma material. The self-directed version — pendulation practice — can be incorporated into daily somatic check-ins: moving attention between a place in the body that feels activated and a place that feels neutral or settled, spending time in each, and noticing how the activated area changes when it is held alongside resource rather than in isolation.
Physical Symptoms During Integration
A frequently unreported aspect of the integration period: physical symptoms often arise in the days and weeks following a session. Fatigue, mild illness, unusual muscle soreness, increased sensitivity to temperature, heightened sensory perception, vivid physical sensations during sleep. These are not coincidental.
The nervous system reorganization initiated by the session continues in the body as well as the mind. Muscles that were braced during intense moments of the session may release over days; this release can feel like soreness or fatigue. The immune system is closely linked to the stress-response system, and periods of significant emotional processing often produce transient immune fluctuations. The heightened interoceptive awareness that persists during the integration window means that physical sensations that were always present become more noticeable.
When physical symptoms require medical attention:
Integration-related physical symptoms are typically mild and self-limiting. Seek medical attention if you experience: chest pain or cardiac symptoms; symptoms that persist beyond two weeks; fever above 38.5°C / 101.3°F; significant neurological symptoms (persistent visual disturbances, numbness, significant coordination difficulty); or any symptom severe enough that you would ordinarily see a doctor.
If you are experiencing HPPD (Hallucinogen Persisting Perception Disorder) — persistent visual disturbances including tracers, halos, or visual snow — this is a real condition that warrants evaluation. It is uncommon, particularly after psilocybin, and typically resolves over weeks to months with appropriate support.
Sleep and Dreams as Integration Material
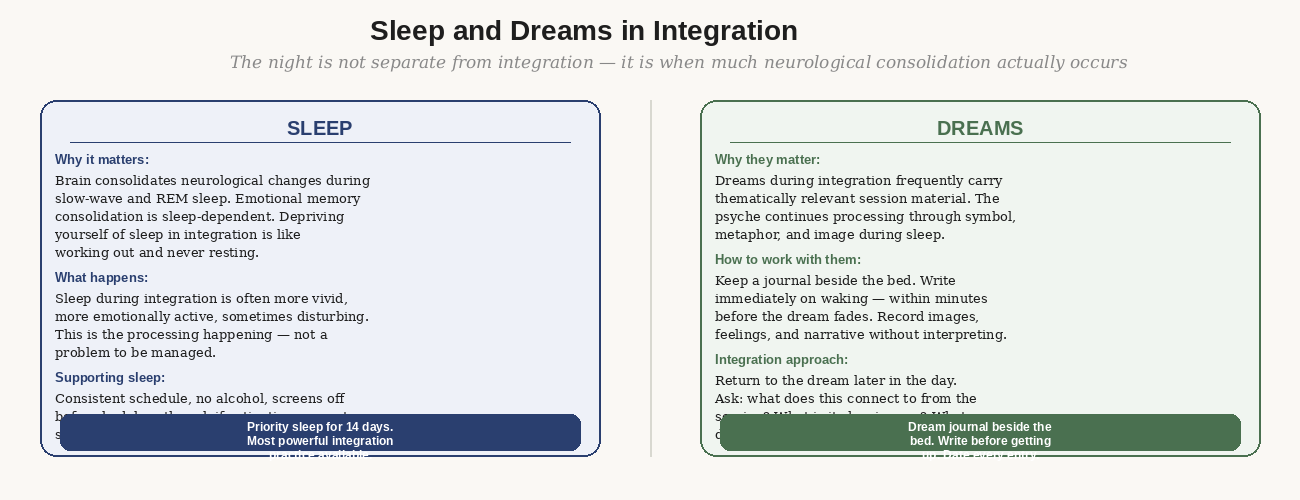
Figure 3: The night is not separate from integration. Sleep consolidates neurological changes; dreams carry integration material in symbolic form.
Sleep as the primary integration mechanism
The neuroscience of memory consolidation is unambiguous: sleep is when the brain processes and consolidates the experiences of the day. During slow-wave sleep, the hippocampus replays recently encoded experiences, strengthening their traces and integrating them into long-term memory. During REM sleep, emotional memories are processed — stripped of their immediate emotional charge while the narrative content is preserved. This is why sleep-deprived people have difficulty regulating emotion and why adequate sleep after significant experiences accelerates integration.
The neurological changes initiated by a psychedelic session are, in part, consolidated during sleep. This is not metaphor — it is the actual mechanism by which the session's neurological disruption becomes stable reorganization. Protecting sleep during the integration period is not a wellness recommendation; it is a direct integration requirement.
Working with dreams
Dreams during the integration period are frequently thematically connected to the session material. The images, situations, and emotional textures of dreams often continue the processing that began during the session, using the brain's natural symbolic language of dream narrative.
The most important practice: write immediately upon waking, before the dream fades. Dreams decay rapidly in the first minutes after waking; what feels vivid at 6:00am is often gone by 6:10am. Keep the journal within reach of the bed and write before getting up, before checking your phone, before speaking. Prioritize images and feelings over narrative coherence — write what you remember, not a polished account.
Later in the day, return to the dream entry and apply the inquiry practice from Module 8: what does this connect to from the session? What is it showing me? What does it ask of me? Dreams often yield their integration content most readily when approached with the same curiosity and openness as the session material itself — not as riddles to be solved but as communications to be received.
The thing people most want to avoid in this module is actually feeling their body during integration.
The mind will generate endless interesting material to work with — insights to revisit, stories to refine, questions to pursue. This is genuinely useful and entirely insufficient. The integration that produces lasting change happens when the nervous system updates, and the nervous system updates through the body, not through the mind thinking about the body.
The daily somatic check-in below takes five minutes. The body map takes twenty. The walking practice takes thirty. None of these feel as productive as a long journaling session or a deep conversation about what the medicine showed you. That feeling of low productivity is the feeling of something that works differently than cognitive processing — not less, differently.
The question to sit with: are you integrating in ways that feel good, or in ways that actually work? Sometimes these overlap. Sometimes the most productive integration is the most uncomfortable — the one that requires putting down the notebook and moving the body.
The Body Map
Time required: 20–30 minutes per session.
Frequency: Weekly across the 30-day integration period — create a new map each week and compare.
Materials: A printout or hand-drawn copy of the body outline, plus colored pens if available.
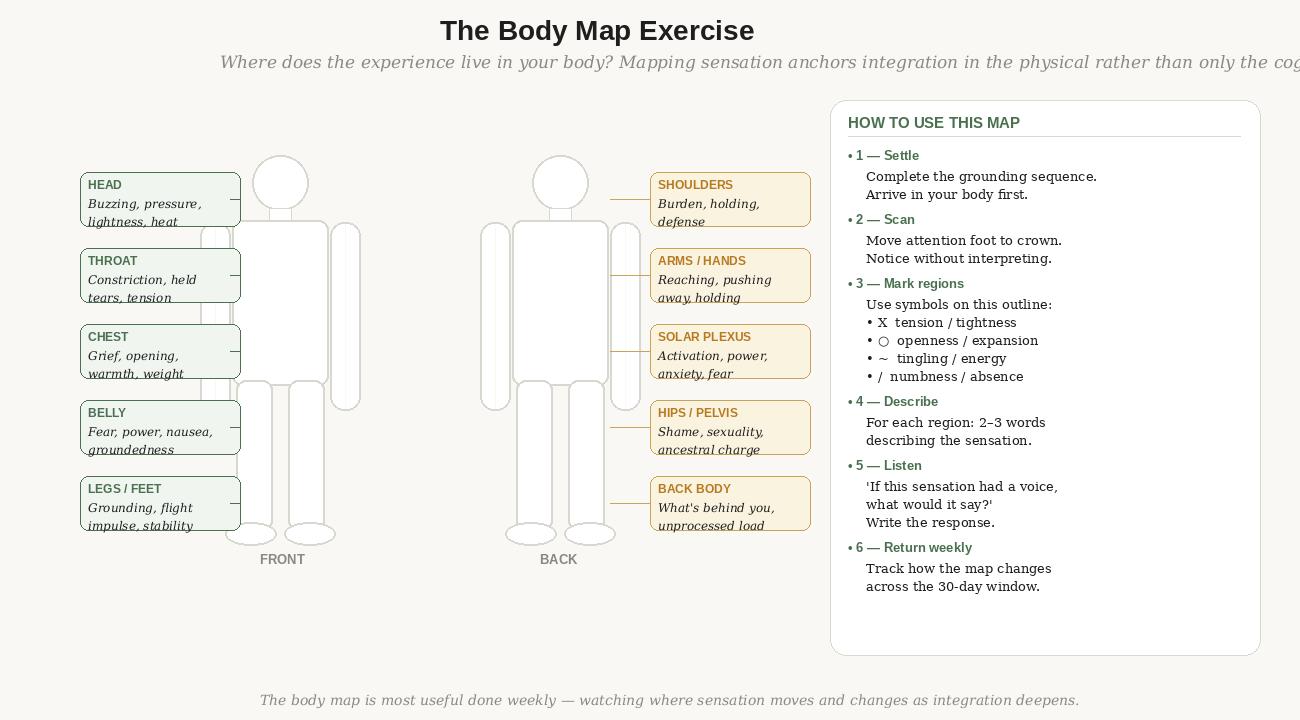
Figure 4: The body map — annotating where sensation lives in the body after the session. Most useful done weekly across the 30-day integration period.
The body map exercise gives the integration material a physical location — which is where it actually lives. It moves integration from the purely cognitive to the somatic by asking the body directly where it is holding the session's residue.
The six-step body map protocol
- Settle: Complete the somatic grounding sequence from Module 4. This is not optional — arriving in the body before beginning the scan changes what you find. Take at least two minutes.
- Scan: Move attention slowly from your feet to the crown of your head. At each region, pause for five to ten seconds. Notice without interpreting. What is there?
- Mark: On your body map, mark each region where you notice significant sensation. Use the following symbols: X for tension or tightness, ○ for openness or expansion, ~ for tingling or energy, / for numbness or absence of sensation.
- Describe: For each marked region, write two to three words describing the sensation — not what you think it means, just what it feels like. "Heavy, pressing, warm." "Buzzing, light, expansive." "Empty, hollow, still."
- Listen: For the region carrying the most charge — the one that feels most significant or most uncomfortable — stay with it for sixty seconds. Then ask internally: "If this sensation had a voice, what would it say?" Write whatever comes, without editing.
- Close: Complete the practice by scanning from crown back to feet. Notice whether anything has shifted. Thank the body for its information. This is not performance — the practice of acknowledgment builds the somatic relationship that deeper integration requires.
Using the map across the integration period
Create a new map each week and keep all of them. Reading the maps in sequence — week 1, week 2, week 3, week 4 — often reveals a clear progression: areas of high charge at week 1 that gradually reduce; new areas emerging as earlier ones settle; the mapping of the integration process in somatic terms. This progression is often invisible to the cognitive mind, which tends to experience integration as non-linear and confusing. The body map makes it visible.
The Daily Somatic Check-In
Time required: 5 minutes.
When: First thing upon waking, before your phone, before speaking.
Duration: 30 days minimum.
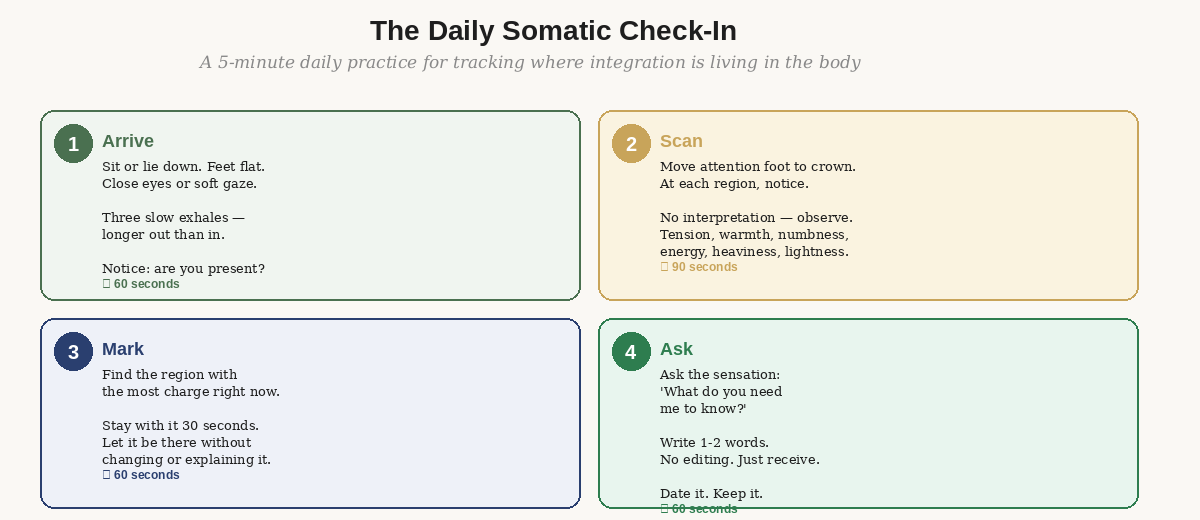
Figure 5: Four steps, five minutes, done before anything else in the morning.
The daily somatic check-in is a shorter version of the body map protocol — compressed for daily use in the integration window. It builds a consistent somatic tracking practice that, over thirty days, creates a granular picture of where integration is occurring and what the body needs on any given day.
Step 1: Arrive (60 seconds)
Before anything else: sit up, feet flat on the floor. Close your eyes or use a soft gaze. Three slow exhales — longer out than in. Notice: are you present? Is attention in the body or already out in the day?
Step 2: Scan (90 seconds)
Move attention from feet to crown. At each region, notice without judgment. You are mapping the terrain, not evaluating it. What is there today that was not there yesterday? What has changed? What persists?
Step 3: Mark (60 seconds)
Identify the region carrying the most sensation or charge right now. Stay with it. Don't try to change it or understand it — simply let it be there while you attend to it. If the sensation shifts or moves, follow it.
Step 4: Ask (60 seconds)
To the region with the most charge, ask: "What do you need me to know today?" Write the response in your integration journal — one to three words, without editing. Date the entry. Over thirty days, these brief somatic reports will constitute a detailed record of how integration has moved through your body.
- Have you completed your first body map? What region carried the most charge, and what did it say when you asked?
- Have you established the daily somatic check-in? If it has felt difficult to maintain, what is getting in the way — and is that obstacle itself integration material?
- Of the five somatic tools, which two are you most committed to using in the coming weeks? What does your choice reveal about what your body is currently asking for?
- Have you protected sleep in the first two weeks? If not — what needs to change this week?
- Have you been working a dream journal? If not, what would it take to set one up tonight?
Resources
Books
Waking the Tiger — Peter Levine. The foundational text on Somatic Experiencing. Chapters 5–8 are most directly relevant to the somatic integration practices in this module.
The Body Keeps the Score — Bessel van der Kolk. Part IV covers somatic and body-based approaches to trauma healing in clinical depth.
Unshakeable — Judith Blackstone. Less well-known than the others but particularly relevant for the relational and embodiment dimensions of integration — especially the pendulation practice.
Research
Berceli, D. (2008). The Revolutionary Trauma Release Process. The primary reference for TRE — includes the original exercises and the neurological rationale.
Walker, M. (2017). Why We Sleep. The most accessible comprehensive treatment of sleep neuroscience — particularly relevant to the consolidation of emotional memories during REM sleep.
Practitioners and training
Somatic Experiencing International (traumahealing.org) — SE practitioner directory, organized by location and specialty. SE-trained practitioners are among the most effective integration support providers for body-held trauma material.
TRE for All (treforall.com) — TRE provider directory and self-learning resources. Many providers offer online sessions for people without local access.